Image Gallary:



Imaging findings:
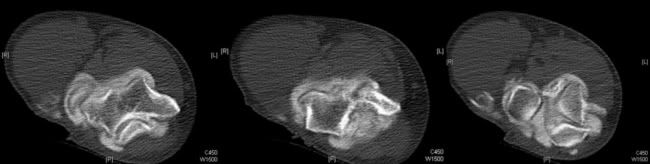
CT scan showed marked narrowing of the joint space with excessive bone formation in and around the elbow joint. Few loose bodies were also shown in the superior aspect of the joint. In addition, calcification was demostrated along the common extensor origin, which is suggestive of calcific lateral epicondylitis.
Discussion:
Osteoarthtitis of the elbow:
Osteoarthritis of the elbow joint is not common. Primary osteoarthitis is almost exclusively seen in men. Although trauma is one of the causes for the osteoarthritis of the elbow joint, many times history of trauma is not elicited. Injury to the ligaments resulting in an unstable elbow can also lead to arthritis, even if the elbow surface is not damaged. For example, professional baseball pitchers place unusually high demands on their throwing elbows.
Plain radiographs usually show spurs at the anterior end of the coronoid and posterior margin of olecranon. CT or MRI are used to differentiate loose bodies from osteophytes. Loss of articular cartilage is common in radiohumeral joint than ulnohumeral joint. Chondral defects tend to occur in the posterolateral aspect of the trochlear notch in sports related osteoarthritis.
Intially the degenerative joint is managed conservatively. Surgical options include arthoscopic debridement, interpostion arthroplasty (tendon or fascia between articular surfaces), radial head excision, orthodesis and elbow joint replacement.
Calcific lateral epicondylitis:
Lateral epicondylitis is a very common overuse syndrome and has many acronyms, viz., tennis elbow, plasterer's elblow, mechanic's elblow, painter's elbow. It is due to overusage of the common extensors of the elbow. According to Nirschl and Pettrone it is due to microscopic tears and reparative tissue in the origin of the extensor carpi radialis brevis (ECRB) muscle. Nirschl also staged the injury: Stage 1 - reversible inflammatory changes. Stage 2 - non-reversible in the origin of the ECRB, Stage 3 - rupture of ECRB, Stage 4 - secondary changes like fibrosis or calcification (calcific lateral epicondylitis)
Plain radiographs may show osteophytes over the lateral epicondyle, calcification close to the lateral epicondyle.
US of the common extensor tendon had high sensitivity but low specificity in the detection of symptomatic lateral epicondylitis
MR is used frequently in the evaluation. Tendinosis is seen as a thickening of the tendon with intermediate signal on T1WI. Mucoid degenerations show high signal T2WI. Coronal or oblique coronal cuts are helpful in the assessment.
CT is not used in the evaluation of the lateral epicondylitis and in the present case it was incidentally diagnosed.
References:
Teh J et al. Imaging of the elbow. Imaging 15:193-204 (2003)
Levin D et al. Lateral Epicondylitis of the Elbow: US Findings. Radiology 2005;237:230-234