Provides anchoring structures for glenohumeral ligaments and the long head of biceps
Divided into superior (12), inferior (6), anterior (9) and posterior (3) portions (brackets are for clock positions)
Anatomy and MRI appearances:
Low signal on all sequences; T2 helpful to distinguish magic angle effects
Sagittal images show the labrum
Superior and inferior labra are best seen on coronals
Superior labrum:
Attached to superior glenoid by loose connective tissue fibres
Provides attachment for long head of bicpes as bicpes anchor
In most the bicpes anchor is attached to posterior superior glenoid with very few fibres attached to anterior labrum; In 50% biceps anchor directly arises from superior labrum with remaining fibres attached to supraglenoid tubercle; Variations in attachement of biceps anchor: entirely posterior in 22%, posterior dominant in 33%, equal in 37% and anterior in 8%
Triangular on coronal and rounded on sagittal
Inferior labrum:
Attached to glenoid by inelastic fibrous tissue
Anterior and posterior labra are best seen on axials
Anterior labrum:
Attached to middle and inferior glenohumeral ligaments
Rounded on axial
Posterior labrum:
Triangular on axial
NORMAL VARIANTS:
Sublabral recess and biceps anchor:
Due to loose attachement of superior labrum
Contrast is seen tracking medially towards glenoid and seen as thin high signal rather than rounded as seen in labral tears and does not extend beyond the origin of biceps anchor
Sublabral foramen:
Seen between 1-3 O clock position and indicates no attachement of anterosuperior labrum to glenoid and usually does not extend beyond 3-4 O clock position
Best seen on coronal or sagittal images where labrum is seen seperated from the glenoid, but reattaches as smooth labral slip at 3 O clock position; on axials the attachment is seen at the level of corocoid
Buford complex:
Seen in 2%
Congenitally absent anterosuperior labrum with thickening of middle glenohumeral ligament
Best seen on sagittal as ;abrum originating at 3 O clock position without labral slip and thick cord likel MGHL
Articular surface undercutting:
Glenoid articular cartilage is interposed between glenoid cortexd and labrum
Tracks medially and may be seen as a less intense than contrast
Ultrasound:
Triangular homogeneously hyperechoic structure with thin (less than 2mm) hypoechoic area at labral base Easily seen in joint effusion.
Anterior labrum: 5MHz curilinear transducer; Anterior or axillary transverse approach in arm adduction or Supine with arm abducted 90° with elbow flexed
Posterior labrum: Posterior transverse scan at level of infraspinatus tendon
Superior labrum: Difficult to see
References:
1. Martinoli C et al. US of the Shoulder: Non–Rotator Cuff Disorders. Radiographics. 2003;23:381-401
2. Robinson G et al. Normal anatomy and common labral lesions at MR arthrography of the shoulder. Clin Rad 61 (805-821)
Image gallery:
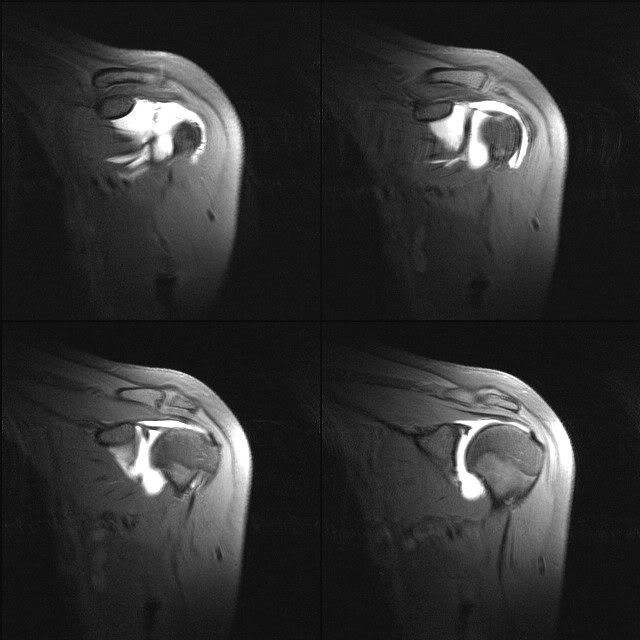
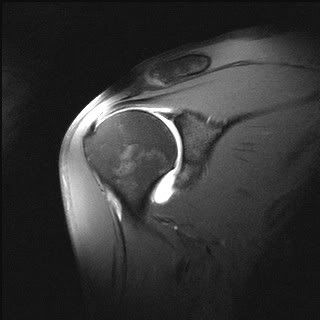
Superior labrum coronal: triangular in shape

Inferior labrum coronal:

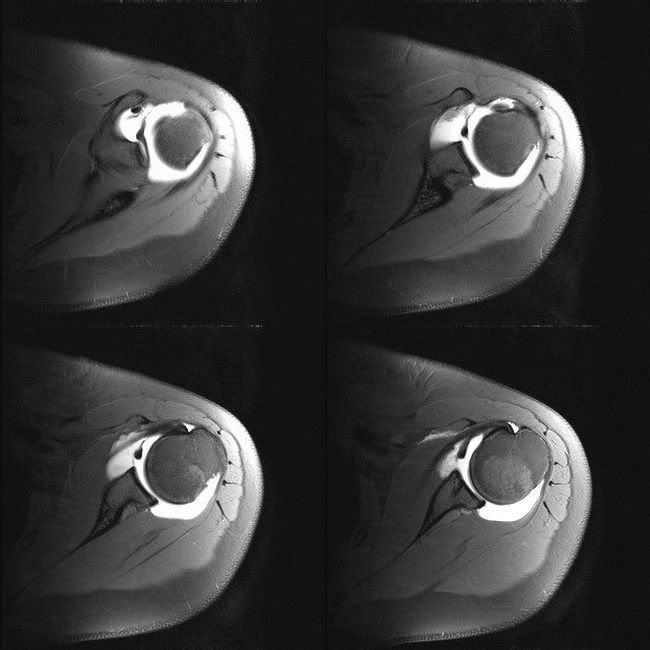
Anterior labrum axial: rounded on axial
Posterior labrum axial: triangular on axial
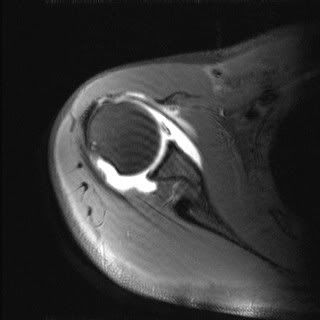
Biceps anchor and sublabral recess:
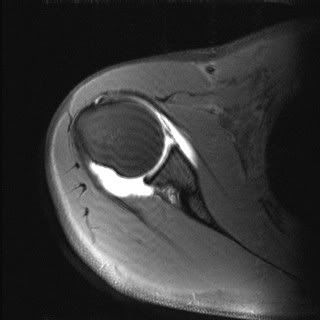
Buford complex: