Acute less than 2 weeks
Chronic more than 2 weeks
Mechanism:
Common in basketball and volleyball players
Due to malialignment
Common in adults
Pathology:
Patellar insertion (proximal tendon) more often than tibial insertion
Posterior surface more prone than superficial
Medial side more common than lateral side
USG:
Disruption of normal fibrillary pattern, swelling, hypoechoes, calcium, hypervascularity
Paratenonitis seen as thickening with echopoor area peripherally
MRI:
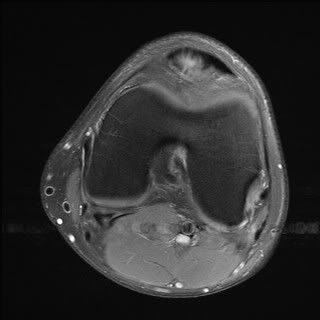
Best seen on sag and axials
Intermediate signal on T1, high on T2 and STIR, may enhance on Gd
Edema in the inferior patella
Focal thickening (convex posterior margin)
Poorly defined posterior margin
Management:
Conservative.
Surgery, if failed conservative treatment, cystic or mucoid degreneration, osteophytosis.
USG guided autologous blood injection, sclerosant injection can be used to treat hypervascular tendinopathies.
USG guided steroid, if marked Hoffitis.
References:
1. Peace KAL et al. Imaging the infrapatellar tendon in the elite athlete. Clin Rad (2006) 61, 570-578
2. Stoller DW. MRI in orthopaedics & sports medicine; Second edition; 1997. Chapter 7: the knee. Lippincott Williams & Wilkins.
Journal watch: Click Here
Image Gallery:
Thick patellar tendon:
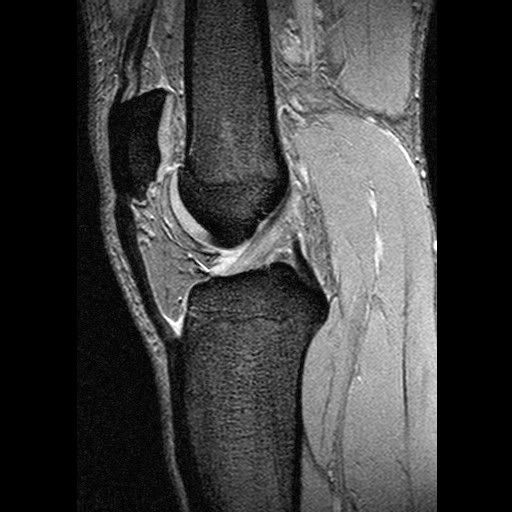
Significantly thickened patellar tendon:

Signal change in the inferior pole of patella:

Associated Hoffa's fat inflmmation:

Convexity and high signal in the medial aspect of the posterior part of the patellar tendon: