Rare focal neural lesion
Slowly progressive painless mononeuropathy
Onion bulb–shaped whorls of neoplastic perineural cell proliferation
On ultrasound it appears hypoechoic with mildly elongated fusiform enlargement of the involved nerve
Reference:
Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
Normal appearances of MSK structures
MUSCLES:
Normal anatomy:
Fibers are grouped into fascicles separated by perimysium (fibrous tissue). The whole muscle is enclosed in epimysium.
Ultrasound:
Transverse - perimysium seen as echogenic dots or short lines scattered throughout the hypoechoic muscle fibre bulk. Intra and intermuscular septae are echogenic
Longitudinal - perimysium seen as oblique parallel echogenic stripe against hypoechoic muscle.
Dynamic scan - During contraction, muscle alters the shape and is hypoechoic with increased angulation of septae
Artefact - Beware of anisotropy, which results in marked hypoechogenicity, mimicing tear. To avoid this keep the transducer perpendicular to the muscle
TENDON:
Ultrasound:
Beware of anisotrophy all the time
Tendons are hyperechoic
LIGAMENTS:
Ultrasound:
Ligaments are hypoechoic
NERVE:
Ultrasound:
Multiple longitudinal hypoechoic bands representing fascicular bundles; separated by discontinuous bands of increased echogenicity, representing surrounding epineurium
References:
1. Lee JC et al. Sonography of Lower Limb Muscle Injury. AJR 2004; 182:341-351
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
Normal anatomy:
Fibers are grouped into fascicles separated by perimysium (fibrous tissue). The whole muscle is enclosed in epimysium.
Ultrasound:
Transverse - perimysium seen as echogenic dots or short lines scattered throughout the hypoechoic muscle fibre bulk. Intra and intermuscular septae are echogenic
Longitudinal - perimysium seen as oblique parallel echogenic stripe against hypoechoic muscle.
Dynamic scan - During contraction, muscle alters the shape and is hypoechoic with increased angulation of septae
Artefact - Beware of anisotropy, which results in marked hypoechogenicity, mimicing tear. To avoid this keep the transducer perpendicular to the muscle
TENDON:
Ultrasound:
Beware of anisotrophy all the time
Tendons are hyperechoic
LIGAMENTS:
Ultrasound:
Ligaments are hypoechoic
NERVE:
Ultrasound:
Multiple longitudinal hypoechoic bands representing fascicular bundles; separated by discontinuous bands of increased echogenicity, representing surrounding epineurium
References:
1. Lee JC et al. Sonography of Lower Limb Muscle Injury. AJR 2004; 182:341-351
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
Muscle injury
Normal anatomy:
Fibers are grouped into fascicles separated by perimysium (fibrous tissue). The whole muscle is enclosed in epimysium.
Normal ultrasound appearance:
Transverse - perimysium seen as echogenic dots or short lines scattered throughout the hypoechoic muscle fibre bulk. Intra and intermuscular septae are echogenic
Longitudinal - perimysium seen as oblique parallel echogenic stripe against hypoechoic muscle. During contraction, muscle alters the shape and is hypoechoic with increased angulation of septae
Beware of anisotropy, which results in marked hypoechogenicity, mimicing tear. To avoid this keep the transducer perpendicular to the muscle
Strains:
Grading (clinical, sonographic and MRI):
I - Spasm or cramp, stiff & sore, rapid recovery without loss of muscle strength, managed conservatively
USG - normal or focal/ generalalized) area of hyperechogenicity with or without perifascial fluid
MRI - edema/hemorrhave/both with normal muscle morphology
II - Overuse, resolve with rest, include intrasubstance tear and partial detachment of muscle from adjacent fascia or aponeurosis. Present with pain and loss of function.
USG - discontinuity of muscle fibers in echogenic perimysial striae, hypervascular, intramuscular fluid. Dynamic scanning may enhance the size and contrast of the lesion (e.g., tennis leg - medial head of gastrocnemius detaches from its common aponeurosis with soleus)
MRI - edema/hemorrhage with tear and disruption up to 50%
III - Complete myotendinous or tendoosseous tear with avulsion/retraction. Due to violent contraction against firm resistance. Early surgery may be required
USG - complete discontinuity of muscle fibers, associated hematoma. Clapper in bell sign refers to retracted echogenic muscle fragments surrounded by hypoechoic hematoma
US is superior to MR in differentiating grade 2 from 1 strains.
MRI - complete tear with retraction
Contusion:
Ill-defined hyperechogenicity in the muscle, which may cross fascial boundaries. Associated with swollen muscle.
Hematoma:
Hypoechoic fluid and may contain debris
Scar:
Hyperechoic heterogeneous, linear/stellate lesion adherent to epimysium and not change with contraction
Hernia:
Through weak aponeurosis or fascia. Hernia is better demonstrated during dynamic scan.
Myositis ossificans:
Hypoechoic mass with sheets of echogenic material and later, coarse calcifications often parallel to adjacent diaphysis
References:
1. Lee JC et al. Sonography of Lower Limb Muscle Injury. AJR 2004; 182:341-351
Image Gallery:
MR: Grade I muscle strain:
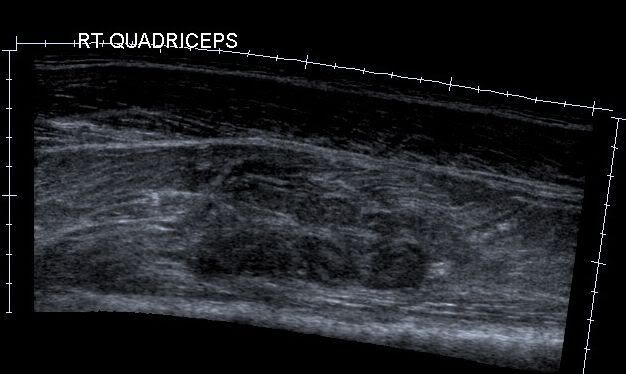
Hematoma in quadriceps:
Fibers are grouped into fascicles separated by perimysium (fibrous tissue). The whole muscle is enclosed in epimysium.
Normal ultrasound appearance:
Transverse - perimysium seen as echogenic dots or short lines scattered throughout the hypoechoic muscle fibre bulk. Intra and intermuscular septae are echogenic
Longitudinal - perimysium seen as oblique parallel echogenic stripe against hypoechoic muscle. During contraction, muscle alters the shape and is hypoechoic with increased angulation of septae
Beware of anisotropy, which results in marked hypoechogenicity, mimicing tear. To avoid this keep the transducer perpendicular to the muscle
Strains:
Grading (clinical, sonographic and MRI):
I - Spasm or cramp, stiff & sore, rapid recovery without loss of muscle strength, managed conservatively
USG - normal or focal/ generalalized) area of hyperechogenicity with or without perifascial fluid
MRI - edema/hemorrhave/both with normal muscle morphology
II - Overuse, resolve with rest, include intrasubstance tear and partial detachment of muscle from adjacent fascia or aponeurosis. Present with pain and loss of function.
USG - discontinuity of muscle fibers in echogenic perimysial striae, hypervascular, intramuscular fluid. Dynamic scanning may enhance the size and contrast of the lesion (e.g., tennis leg - medial head of gastrocnemius detaches from its common aponeurosis with soleus)
MRI - edema/hemorrhage with tear and disruption up to 50%
III - Complete myotendinous or tendoosseous tear with avulsion/retraction. Due to violent contraction against firm resistance. Early surgery may be required
USG - complete discontinuity of muscle fibers, associated hematoma. Clapper in bell sign refers to retracted echogenic muscle fragments surrounded by hypoechoic hematoma
US is superior to MR in differentiating grade 2 from 1 strains.
MRI - complete tear with retraction
Contusion:
Ill-defined hyperechogenicity in the muscle, which may cross fascial boundaries. Associated with swollen muscle.
Hematoma:
Hypoechoic fluid and may contain debris
Scar:
Hyperechoic heterogeneous, linear/stellate lesion adherent to epimysium and not change with contraction
Hernia:
Through weak aponeurosis or fascia. Hernia is better demonstrated during dynamic scan.
Myositis ossificans:
Hypoechoic mass with sheets of echogenic material and later, coarse calcifications often parallel to adjacent diaphysis
References:
1. Lee JC et al. Sonography of Lower Limb Muscle Injury. AJR 2004; 182:341-351
Image Gallery:
MR: Grade I muscle strain:
Hematoma in quadriceps:
Para-acetabular insufficiency fractures
Cooper et al (1985)
Associated with other pelvic insufficiency fractures
Causes include porosis, RA, RTP, steroids
Clinical features: severe hip and pelvic pain
Radiography:
Limited value, poor sensitivity
Band like or patchy subchondral sclerosis in paraacetabular area
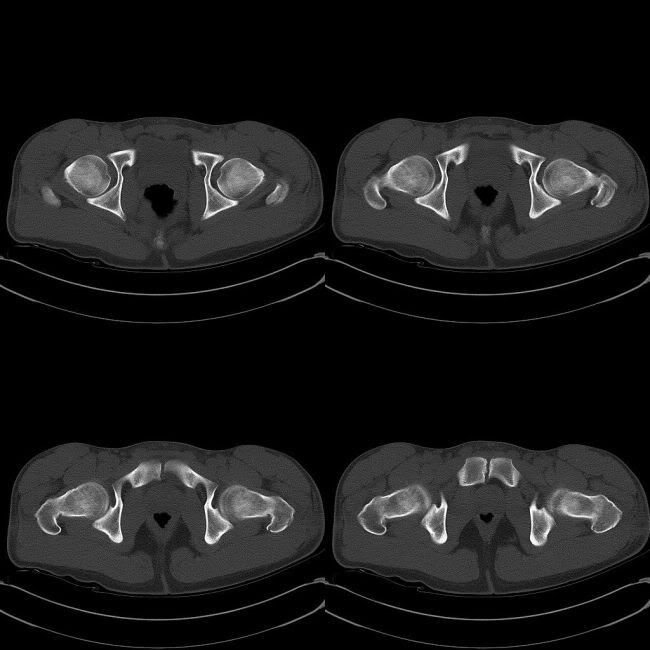
CT:
Condensed sclerotic bone
Bone scintigraphy:
Intense tracer uptake in para-acetabular region
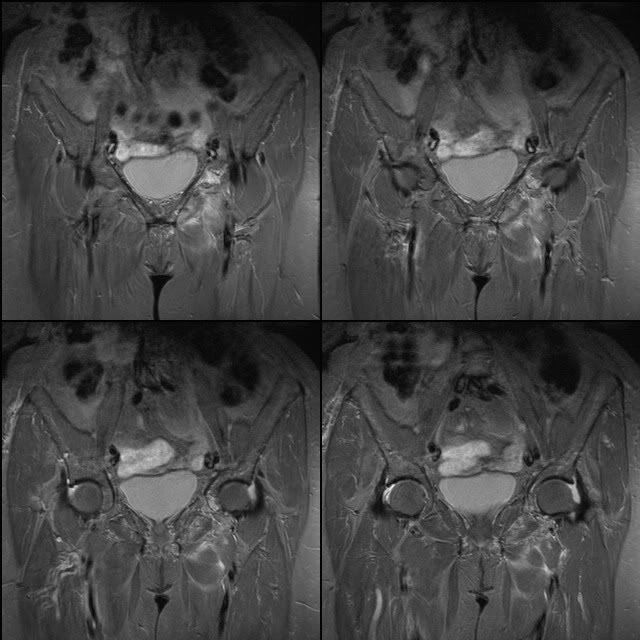
MRI:
Fracture seen as band of low signal on T1 and T2, surrounded by marrow edema seen as low signal on T1 and high signal on T2
Fracture line - curvilinear and parallel to acetabular roof, striaght and crossing acetabular roof in oblique way
Marked enhancement of adjacent area on Gd
References:
Theodorou SJ et al. Magnetic resonance imaging of para-acetabular insufficiency fractures in patients with malignancy . Clin Rad 2006: 181-190
Associated with other pelvic insufficiency fractures
Causes include porosis, RA, RTP, steroids
Clinical features: severe hip and pelvic pain
Radiography:
Limited value, poor sensitivity
Band like or patchy subchondral sclerosis in paraacetabular area
CT:
Condensed sclerotic bone
Bone scintigraphy:
Intense tracer uptake in para-acetabular region
MRI:
Fracture seen as band of low signal on T1 and T2, surrounded by marrow edema seen as low signal on T1 and high signal on T2
Fracture line - curvilinear and parallel to acetabular roof, striaght and crossing acetabular roof in oblique way
Marked enhancement of adjacent area on Gd
References:
Theodorou SJ et al. Magnetic resonance imaging of para-acetabular insufficiency fractures in patients with malignancy . Clin Rad 2006: 181-190
Vertebral compression fractures
Malignant compression fractures:
Morhological features:
Convex bulge involving posterior cortex (70% sensitive and 94% specific)
Involvement of pedicles (80% sensitive and 94% specific)
Presence of epidural (80% sensitive and 100% specific) mass
Paraspinal soft tissue
Signal:
T1-diffuse low signal
T2-iso-to-high signal
Enhance post Gd
Benign compression fractures:
Morphological features:
Retropulsion of posterior fragment (often posterosuperior) (100% specific, 16% sensitive)
Signal features:
T1 - focal band of low signal adjacent to end plate
T2 - overall vertebra is iso with adjacent non-fractured bone with focal low signal band of fracture
STIR - 'fluid sign' - linear or traingular area of high signal adjacent to endplate - in acute and subacute compression fractures and rarely seen in malignant fractures
Post Gd - 'return of normal signal', i.e., enhances same as adjacent vertebrae
At least one normal signal area is seen, usually opposite the fractured end plate
Gradually return to normal signal as adjacent vertebrae with aging (after 2-4 months)
Vacuum cleft is suggestive of benign pathology, seen as low signal on T1, low signal (before 10 min of supine) or high signal (after 10 min supine) on T2
References:
Uetani M et al. Malignant and benign compression fractures: differentiation and diagnostic pitfalls on MRI . Clin Rad 2004: 124-131
Morhological features:
Convex bulge involving posterior cortex (70% sensitive and 94% specific)
Involvement of pedicles (80% sensitive and 94% specific)
Presence of epidural (80% sensitive and 100% specific) mass
Paraspinal soft tissue
Signal:
T1-diffuse low signal
T2-iso-to-high signal
Enhance post Gd
Benign compression fractures:
Morphological features:
Retropulsion of posterior fragment (often posterosuperior) (100% specific, 16% sensitive)
Signal features:
T1 - focal band of low signal adjacent to end plate
T2 - overall vertebra is iso with adjacent non-fractured bone with focal low signal band of fracture
STIR - 'fluid sign' - linear or traingular area of high signal adjacent to endplate - in acute and subacute compression fractures and rarely seen in malignant fractures
Post Gd - 'return of normal signal', i.e., enhances same as adjacent vertebrae
At least one normal signal area is seen, usually opposite the fractured end plate
Gradually return to normal signal as adjacent vertebrae with aging (after 2-4 months)
Vacuum cleft is suggestive of benign pathology, seen as low signal on T1, low signal (before 10 min of supine) or high signal (after 10 min supine) on T2
References:
Uetani M et al. Malignant and benign compression fractures: differentiation and diagnostic pitfalls on MRI . Clin Rad 2004: 124-131
Tarsal coalition
Bony/ cartilaginous/ fibrous union between two or more bones of foot
1% of population
90% are calcaneonavicular (CN) or talocalcaneal (middle facet) (TC). CN coalition presents in childhood, where as TC present in early adulthood
Restrict subtalar eversion, inversion and anterior gliding, may cause flatfoot, pain, tarsal tunnel syndrome, tenderness, peroneal tendon spasm
Usually present in second decade of life
AD pattern is suggested
Biltaeral in about 50%
Common in rigid or spastic flatfoot
Nuclear imaging may show increased uptake
MR may show adjacent marrow edema
Usually treated conservatively with orthotics, casting, NSAID, steroid injections, physiotherapy. Surgucal options for calcaneonavicular coalition include resection with or without extensor digitorum brevis interposition, triple arthrodesis; and for talocalcaneal coalition include middle facet bony bridge resection with fat interposition, triple arthrodesis
Talocalcaneal (subtalar) coalition:
Subtalar joint consits of anterior, middle and posterior facets
AP, lateral and 45 degree internal oblique views
C sign: continuous arc between medial talar cortex and inferior cortex of sustentaculum tali on lateral radiograph. Most sensitive.
Talar beak sign: flaring of superior margin of talar head on lateral radiograph. Similar variants are hooklike osteophyte of talar head (in OA) and talar ridge (occurs more proximally)
Nonvisualized middle facet: indicated subtalar coalition on lateral view
Dysmorphic sustentaculum tali: ovoid on lateral radiograph. Normal is flat brick shaped
Other signs include: narrowing of posterior subtalar joint, rounding of lateral talar process, ball-in-socket configuration of talus
CT: coronal CT shows bony bar in middle facet of subtalar joint. In nonosseous coalition, middle facet may be narrow. Normally, sustentaculum slopes upward medially; in talocalcaneal coalition it slopes generally downward or horizontally. Sustentaculum may be broad or hypoplastic
MRI: coronal plane is best
Calcaneonavicular coalition:
Best seen on 45 degree internal oblique view. Calcaneus and navicular do not articulate.
AntEater sign: broad and elongated anterior process of calcaneus on lateral or AP radiograph. To be distinguished from normal triangular configuration of anterior process. Most sensitive sign Calcaneonavicular bar: visible bony bar or an anomalous articulation between navicular and calcaneus seen on Ap radiograph
Wide navicular: proximal articular cortex of navicular wider than articular cortex of talar head
Tapered elongated navicular: on AP view
Wide or flat anteromedial calcaneus: on AP oblique
Hypoplasia of talus: may be seen
CT:axial CT shows broadening of medial aspect of anterior and dorsal calcaneus near navicular
MRI: best on sagittal and axial MR. Sagittal images show orientation of calcaneonavicular bridging. Elongated anterior dorsal calcaneus, anteater's nose, may be seen on only one image.
References:
1. Crim JR et al. Radiographic Diagnosis of Tarsal Coalition . AJR 2004; 182:323-328
2. Joel S. Newman and Arthur H. Newberg. Congenital Tarsal Coalition: Multimodality Evaluation with Emphasis on CT and MR Imaging : RadioGraphics 2000; 20: 321
Image Gallary:
Normal lateral view: There is no C sign, no talar beak, brick shaped sustentaculum tali

Normal foot oblique view: no 'anteater sign', no talar beak, normal middle facet, normal articular cortex of navicular

1% of population
90% are calcaneonavicular (CN) or talocalcaneal (middle facet) (TC). CN coalition presents in childhood, where as TC present in early adulthood
Restrict subtalar eversion, inversion and anterior gliding, may cause flatfoot, pain, tarsal tunnel syndrome, tenderness, peroneal tendon spasm
Usually present in second decade of life
AD pattern is suggested
Biltaeral in about 50%
Common in rigid or spastic flatfoot
Nuclear imaging may show increased uptake
MR may show adjacent marrow edema
Usually treated conservatively with orthotics, casting, NSAID, steroid injections, physiotherapy. Surgucal options for calcaneonavicular coalition include resection with or without extensor digitorum brevis interposition, triple arthrodesis; and for talocalcaneal coalition include middle facet bony bridge resection with fat interposition, triple arthrodesis
Talocalcaneal (subtalar) coalition:
Subtalar joint consits of anterior, middle and posterior facets
AP, lateral and 45 degree internal oblique views
C sign: continuous arc between medial talar cortex and inferior cortex of sustentaculum tali on lateral radiograph. Most sensitive.
Talar beak sign: flaring of superior margin of talar head on lateral radiograph. Similar variants are hooklike osteophyte of talar head (in OA) and talar ridge (occurs more proximally)
Nonvisualized middle facet: indicated subtalar coalition on lateral view
Dysmorphic sustentaculum tali: ovoid on lateral radiograph. Normal is flat brick shaped
Other signs include: narrowing of posterior subtalar joint, rounding of lateral talar process, ball-in-socket configuration of talus
CT: coronal CT shows bony bar in middle facet of subtalar joint. In nonosseous coalition, middle facet may be narrow. Normally, sustentaculum slopes upward medially; in talocalcaneal coalition it slopes generally downward or horizontally. Sustentaculum may be broad or hypoplastic
MRI: coronal plane is best
Calcaneonavicular coalition:
Best seen on 45 degree internal oblique view. Calcaneus and navicular do not articulate.
AntEater sign: broad and elongated anterior process of calcaneus on lateral or AP radiograph. To be distinguished from normal triangular configuration of anterior process. Most sensitive sign Calcaneonavicular bar: visible bony bar or an anomalous articulation between navicular and calcaneus seen on Ap radiograph
Wide navicular: proximal articular cortex of navicular wider than articular cortex of talar head
Tapered elongated navicular: on AP view
Wide or flat anteromedial calcaneus: on AP oblique
Hypoplasia of talus: may be seen
CT:axial CT shows broadening of medial aspect of anterior and dorsal calcaneus near navicular
MRI: best on sagittal and axial MR. Sagittal images show orientation of calcaneonavicular bridging. Elongated anterior dorsal calcaneus, anteater's nose, may be seen on only one image.
References:
1. Crim JR et al. Radiographic Diagnosis of Tarsal Coalition . AJR 2004; 182:323-328
2. Joel S. Newman and Arthur H. Newberg. Congenital Tarsal Coalition: Multimodality Evaluation with Emphasis on CT and MR Imaging : RadioGraphics 2000; 20: 321
Image Gallary:
Normal lateral view: There is no C sign, no talar beak, brick shaped sustentaculum tali
Normal foot oblique view: no 'anteater sign', no talar beak, normal middle facet, normal articular cortex of navicular
Malignant peripheral nerve sheath tumours
5-10% of soft tissue tumours
20-50 years of age
Most commonly involve major nerves like sciatic nerve, brachial plexus and sacral plexus
20-50 years of age
Most commonly involve major nerves like sciatic nerve, brachial plexus and sacral plexus
Neurofibromatosis
1 in 3000 births
AD with high penetrance, 50% new mutations
Advanced paternal age (more than 35) is a risk factor
Mesodermal dysplasia
Chr-17
Triad of Café-au-lait spots (90%), skeletal deformity and mental deficiency
Axillary or inguinal freckling, optic glioma, Lisch nodules (iris hamartomas)
Bone lesions: (25-40%)
Facial/ orbital/ sphenoid dysplasia
Pseudarthrosis, tibia is common
Scoliosis, Kyphosis
Lambdoid suture defects, usually left side
Periosteal reaction
Multiple nonossifying fibromas or fibroxanthomas
Ribbon ribs
Posterior scalloping of the vertebrae due to dural ectasia
Neural lesions:
All three types of neurofibromas - localized, diffuse and plexiform - are associated
Localized neurofibroma is most common type, plexiform is pathgnomonic (may cause elephantiasis neuromatosa)
Malignant transformation 2-30%
Treatment:
Often non-surgical
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
AD with high penetrance, 50% new mutations
Advanced paternal age (more than 35) is a risk factor
Mesodermal dysplasia
Chr-17
Triad of Café-au-lait spots (90%), skeletal deformity and mental deficiency
Axillary or inguinal freckling, optic glioma, Lisch nodules (iris hamartomas)
Bone lesions: (25-40%)
Facial/ orbital/ sphenoid dysplasia
Pseudarthrosis, tibia is common
Scoliosis, Kyphosis
Lambdoid suture defects, usually left side
Periosteal reaction
Multiple nonossifying fibromas or fibroxanthomas
Ribbon ribs
Posterior scalloping of the vertebrae due to dural ectasia
Neural lesions:
All three types of neurofibromas - localized, diffuse and plexiform - are associated
Localized neurofibroma is most common type, plexiform is pathgnomonic (may cause elephantiasis neuromatosa)
Malignant transformation 2-30%
Treatment:
Often non-surgical
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
Nerve sheath ganglion
Most comonly seen in the large nerves about the knee - popliteal, peroneal, tibial - at the level of fibular head
Cystic in nature on imaging
Clinical features:
Palpable mass
Neurologic symptoms due to compression
Treatment:
Excision
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
Cystic in nature on imaging
Clinical features:
Palpable mass
Neurologic symptoms due to compression
Treatment:
Excision
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
Neural fibrolipoma
Mason (1953)
Also called fibrolipomatous hamartoma of nerve, perineural lipoma, fatty infiltration of the nerve, intraneural lipoma, lipomatosis of nerve
Due to infiltration and hypertrophy of mature fibrofatty tissue infiltrating epi and perineurium
Commonly present at birth or early childhood, and most present before 30 years of age
Non-hereditary
Median nerve is most commonly involved (more than 80%). 2nd most common ulnar nerve. Other reported nerves include brachial plexus, radial, peroneal nerves
Usually less than 30 years age
Clinical features:
Soft, slowly enlarging mass in the palmar aspect of the hand, wrist or forearm since childhood
Pain
Neurological symptoms
Associated macrodactyly = macrodystrophia lipomatosa, usually involves 2 and 3rd digits, in 27-67%
Radiography:
Soft-tissue swelling and bone overgrowth, usually of 2 and 3rd digits, may show bowing
Secondary degenerative changes may be seen
Ultrasound:
Alternating hyper and hypoechoic bands (cable appearance) due to elongated and enlarged median nerve
MRI:
Pathognomonic - longitudinally oriented cylindric foci (3 mm diameter) of low signal surrounded by fat signal (cable appearance)
Increased fat in overgrown digits
Thickened median nerve
References:
1. Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
3. Murphey MD et al. Benign Musculoskeletal Lipomatous Lesions. RadioGraphics 2004;24:1433-1466
4. Nouira K et al. Fibrolipoma of the median nerve. Joint bone spine 2007: 74: 98-99
Also called fibrolipomatous hamartoma of nerve, perineural lipoma, fatty infiltration of the nerve, intraneural lipoma, lipomatosis of nerve
Due to infiltration and hypertrophy of mature fibrofatty tissue infiltrating epi and perineurium
Commonly present at birth or early childhood, and most present before 30 years of age
Non-hereditary
Median nerve is most commonly involved (more than 80%). 2nd most common ulnar nerve. Other reported nerves include brachial plexus, radial, peroneal nerves
Usually less than 30 years age
Clinical features:
Soft, slowly enlarging mass in the palmar aspect of the hand, wrist or forearm since childhood
Pain
Neurological symptoms
Associated macrodactyly = macrodystrophia lipomatosa, usually involves 2 and 3rd digits, in 27-67%
Radiography:
Soft-tissue swelling and bone overgrowth, usually of 2 and 3rd digits, may show bowing
Secondary degenerative changes may be seen
Ultrasound:
Alternating hyper and hypoechoic bands (cable appearance) due to elongated and enlarged median nerve
MRI:
Pathognomonic - longitudinally oriented cylindric foci (3 mm diameter) of low signal surrounded by fat signal (cable appearance)
Increased fat in overgrown digits
Thickened median nerve
References:
1. Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
3. Murphey MD et al. Benign Musculoskeletal Lipomatous Lesions. RadioGraphics 2004;24:1433-1466
4. Nouira K et al. Fibrolipoma of the median nerve. Joint bone spine 2007: 74: 98-99
Mortan's neuroma
General points:
Thomas Mortan (1876)
Most common between 3 and 4th metatarsal heads, next common site is between 2-3rd heads
More common in women (high heeled shoes)
Fusiform enlargement of plantar digital nerve at bifurcation with thickened epineural fascicles, perineural fibrosis and loss of the myelinated fibers
Clinical features:
Exercise provoked pain, relieved on rest
Compression in the intermetatarsal space may induce pain
Usually not paplable unless associated with synovial cysts
Usually asymptomatic
Ultrasound:
Round/ oval, well-defined, hypoechoic mass just proximal to metatarsal heads in intermetatarsal space. Less than 5mm lesion difficult to see
Intermetatarsal bursa is on the dorsal aspect
Lateral compression will move the neuroma to the plantar side
Best seen on sagittal axis as a round disc
MRI:
Most evident on coronal T1, best seen on FS Gd T1
Less conspicuous on T2 and difficult to differentiate it from surrounding muscle and fat.
Fat FS T2 useful
Seen centered in neurovascular bundle within intermetatarsal space on plantar side of transverse metatarsal ligament as a well defined (beware of partial volume artifact from adjacent joint capsule) mass with signal similar to skeletal muscle on T1 and less than fat on T2
Intermetatarsal bursal fluid may be seen proximal to Morton neuroma in majority (66%)
Often enhance on Gd
Accuracy of 90%
Treatment:
Modification of footwear, neurolysis, steroid injection, ultrasound therapy
Ultrasound guided steroid/LA injection, alcohol injection
Surgical dempression by releasing transverse metatarsal ligament
Surgical resection of neuroma and involved nerve segment
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
JOURNAL WATCH:
Alcohol injection under ultrasound guidance is highly effective in Mortan's neuroma
AJR 2007; 188:1535-1539
Hughes et al, in their paper 'Treatment of Morton's Neuroma with Alcohol Injection Under Sonographic Guidance: Follow-Up of 101 Cases', report the technical success of 100%, partial or total symptom improvement in 94%, totally pain free in 84%. Transient increase in pain occurred in 17%. There were no major complications. The decrease in size was by 30%.
Conclusion: Alcohol injection has high success rate, well tolerated and comparable to surgical results.
Thomas Mortan (1876)
Most common between 3 and 4th metatarsal heads, next common site is between 2-3rd heads
More common in women (high heeled shoes)
Fusiform enlargement of plantar digital nerve at bifurcation with thickened epineural fascicles, perineural fibrosis and loss of the myelinated fibers
Clinical features:
Exercise provoked pain, relieved on rest
Compression in the intermetatarsal space may induce pain
Usually not paplable unless associated with synovial cysts
Usually asymptomatic
Ultrasound:
Round/ oval, well-defined, hypoechoic mass just proximal to metatarsal heads in intermetatarsal space. Less than 5mm lesion difficult to see
Intermetatarsal bursa is on the dorsal aspect
Lateral compression will move the neuroma to the plantar side
Best seen on sagittal axis as a round disc
MRI:
Most evident on coronal T1, best seen on FS Gd T1
Less conspicuous on T2 and difficult to differentiate it from surrounding muscle and fat.
Fat FS T2 useful
Seen centered in neurovascular bundle within intermetatarsal space on plantar side of transverse metatarsal ligament as a well defined (beware of partial volume artifact from adjacent joint capsule) mass with signal similar to skeletal muscle on T1 and less than fat on T2
Intermetatarsal bursal fluid may be seen proximal to Morton neuroma in majority (66%)
Often enhance on Gd
Accuracy of 90%
Treatment:
Modification of footwear, neurolysis, steroid injection, ultrasound therapy
Ultrasound guided steroid/LA injection, alcohol injection
Surgical dempression by releasing transverse metatarsal ligament
Surgical resection of neuroma and involved nerve segment
References:
Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280
JOURNAL WATCH:
Alcohol injection under ultrasound guidance is highly effective in Mortan's neuroma
AJR 2007; 188:1535-1539
Hughes et al, in their paper 'Treatment of Morton's Neuroma with Alcohol Injection Under Sonographic Guidance: Follow-Up of 101 Cases', report the technical success of 100%, partial or total symptom improvement in 94%, totally pain free in 84%. Transient increase in pain occurred in 17%. There were no major complications. The decrease in size was by 30%.
Conclusion: Alcohol injection has high success rate, well tolerated and comparable to surgical results.
Peripheral nerve sheath tumours - Shwannomas and neurofibromas
10% of benign soft tissue neoplasms
Derived from Schwann cells
Most common types - Schwannomas (neurilemmomas) and neurofibromas
Others include Traumatic neuroma (stump neuroma), Mortans neuroma, Neural fibrolipoma, Nerve sheath ganglion, Intraneural perineuroma, Malignant peripheral nerve sheath tumors(7-8%)
Difficult to distinguish them with imaging
Rarely show malignant transformation
Common sites - plantar digital nerve in Morton neuroma, median nerve in neural fibrolipoma (associated with macrodactyly), large nerve trunk in benign and malignant PNSTs, nerve sheath ganglion commonly occurs about the knee (cystic appearance)
The most common lesion in Neurofibromatosis 1 is neurofibroma, although neurilemmoma and malignant PNST may be seen
Neurofibroma:
Solitary; multiple as in NF
20-30 years
1. Localised neurofibroma: most common type (90%), usually solitary, not associated with NF1, 2. Usually superficial cutaneous nerves, slow growing, usually less than 5cm
Diffuse neurofibroma: Children and young adult, subcutaneous tissue of head and neck, not associated with NF1
3. Plexiform neurofibroma = NF1
Schwannona = Neurilemmoma:
Benign slow-growing encapsulated tumors of nerve sheath
Most commonly seen in extremities
Highly ordered cellularity of Antoni type A and less cellular areas with myxoid matrix of Antoni type B
20-30 years
Commonly involves spinal and sympathetic nerve roots of head and neck, flexor surfaces of upper and lower limbs (particularly ulnar and peroneal nerves), posterior mediastinum and retroperitoneum
Single, less than 5cm; if multiple, usually associated with NF1
Fusiform in shape, usually well defined
Treated surgically
Theriotically neurilemoma is eccentric and separable from normal nerve. Neurofibroma is intimately related and indistinguishable from normal nerve
Ultrasound:
Most are homogeneous (may be heterogenous) and hypoechoic
Continuity along the nerve is seen in most; may be eccentric to nerve axis
May show posterior acoustic enhancement, target appearance (hyperechoic center and hypoechoic periphery), pseudocystic appearance
Increased flow on Doppler
Several simulate ganglion cysts, but presence of flow on Doppler excludes uncomplicated ganglion cyst
Ancient Schwannoma may calcify
CT:
Well defined non-homogeneous low density mass
May also show target sign, split fat sign
MRI:
Fusiform appearance in periphery, dumbell haped in paraspinal region
Low-signal (similar to muscle) on T1WI
High signal (higher than fat) on T2WI, diffuse neurofibroma is low on T2
Target sign = peripheral high signal rim with central low-to-int signal on T2 (usually not seen in malignanct PNST), represents central fibrous tissue and peripheral myxioid tissue
Fascicular signon T2 and PD - multiple small ringlike structures with peripheral high signal intensity
Split fat sign on T1
Muscle atrophy on T1
May have fluid -fluid level due to hemorrhage
Strongly enhance on Gd
References:
1. Reynolds JR et al.Sonographic Characteristics of Peripheral Nerve Sheath Tumors . AJR 2004; 182:741-744
2. Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280.
Derived from Schwann cells
Most common types - Schwannomas (neurilemmomas) and neurofibromas
Others include Traumatic neuroma (stump neuroma), Mortans neuroma, Neural fibrolipoma, Nerve sheath ganglion, Intraneural perineuroma, Malignant peripheral nerve sheath tumors(7-8%)
Difficult to distinguish them with imaging
Rarely show malignant transformation
Common sites - plantar digital nerve in Morton neuroma, median nerve in neural fibrolipoma (associated with macrodactyly), large nerve trunk in benign and malignant PNSTs, nerve sheath ganglion commonly occurs about the knee (cystic appearance)
The most common lesion in Neurofibromatosis 1 is neurofibroma, although neurilemmoma and malignant PNST may be seen
Neurofibroma:
Solitary; multiple as in NF
20-30 years
1. Localised neurofibroma: most common type (90%), usually solitary, not associated with NF1, 2. Usually superficial cutaneous nerves, slow growing, usually less than 5cm
Diffuse neurofibroma: Children and young adult, subcutaneous tissue of head and neck, not associated with NF1
3. Plexiform neurofibroma = NF1
Schwannona = Neurilemmoma:
Benign slow-growing encapsulated tumors of nerve sheath
Most commonly seen in extremities
Highly ordered cellularity of Antoni type A and less cellular areas with myxoid matrix of Antoni type B
20-30 years
Commonly involves spinal and sympathetic nerve roots of head and neck, flexor surfaces of upper and lower limbs (particularly ulnar and peroneal nerves), posterior mediastinum and retroperitoneum
Single, less than 5cm; if multiple, usually associated with NF1
Fusiform in shape, usually well defined
Treated surgically
Theriotically neurilemoma is eccentric and separable from normal nerve. Neurofibroma is intimately related and indistinguishable from normal nerve
Ultrasound:
Most are homogeneous (may be heterogenous) and hypoechoic
Continuity along the nerve is seen in most; may be eccentric to nerve axis
May show posterior acoustic enhancement, target appearance (hyperechoic center and hypoechoic periphery), pseudocystic appearance
Increased flow on Doppler
Several simulate ganglion cysts, but presence of flow on Doppler excludes uncomplicated ganglion cyst
Ancient Schwannoma may calcify
CT:
Well defined non-homogeneous low density mass
May also show target sign, split fat sign
MRI:
Fusiform appearance in periphery, dumbell haped in paraspinal region
Low-signal (similar to muscle) on T1WI
High signal (higher than fat) on T2WI, diffuse neurofibroma is low on T2
Target sign = peripheral high signal rim with central low-to-int signal on T2 (usually not seen in malignanct PNST), represents central fibrous tissue and peripheral myxioid tissue
Fascicular signon T2 and PD - multiple small ringlike structures with peripheral high signal intensity
Split fat sign on T1
Muscle atrophy on T1
May have fluid -fluid level due to hemorrhage
Strongly enhance on Gd
References:
1. Reynolds JR et al.Sonographic Characteristics of Peripheral Nerve Sheath Tumors . AJR 2004; 182:741-744
2. Murphey MD et al. Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation . Radiographics. 1999;19:1253-1280.
Lipomatous tumours
Classicification:
Soft tissue:
Benign simple lipoma (soft tissue lipoma)
Lipomatosis
Lipoblastoma and lipoblastomatosis
Angiolipoma
Myolipoma
Spindle cell and pleomorphic lipoma
Hibernoma
Tendon sheath lipoma
Synovial lipoma
Liposarcoma
Bone:
Parosteal lipoma
Intraosseus lipoma
Liposclerosing myxofibrous tumor of bone
Liposarcoma of bone
References:
1. Gaskin CM et al. Lipomas, Lipoma Variants, and Well-Differentiated Liposarcomas (Atypical Lipomas): Results of MRI Evaluations of 126 Consecutive Fatty Masses . AJR 2004; 182:733-739
2. Murphey MD et al. Benign Musculoskeletal Lipomatous Lesions. RadioGraphics 2004;24:1433-1466
Soft tissue:
Benign simple lipoma (soft tissue lipoma)
Lipomatosis
Lipoblastoma and lipoblastomatosis
Angiolipoma
Myolipoma
Spindle cell and pleomorphic lipoma
Hibernoma
Tendon sheath lipoma
Synovial lipoma
Liposarcoma
Bone:
Parosteal lipoma
Intraosseus lipoma
Liposclerosing myxofibrous tumor of bone
Liposarcoma of bone
References:
1. Gaskin CM et al. Lipomas, Lipoma Variants, and Well-Differentiated Liposarcomas (Atypical Lipomas): Results of MRI Evaluations of 126 Consecutive Fatty Masses . AJR 2004; 182:733-739
2. Murphey MD et al. Benign Musculoskeletal Lipomatous Lesions. RadioGraphics 2004;24:1433-1466
de Quervain's tenosynovitis
Chronic inflammatory scar with narrowing of fibroosseous tunnel (1cm long) of first extensor compartment (along radial styloid covered by extensor retinaculum and contains APL- abductor pollicis longus and EPB - extensor pollicis brevis tendons)
Causes:
Pregnancy
First 3 months of lactation, likely to be endocrinal
MRI:
Axial images are best
Thickening of tendon sheath of first extensor compartment and diffuse irregular signal intensity in adjacent subcutaneous fat on T1 and T2
Causes:
Pregnancy
First 3 months of lactation, likely to be endocrinal
MRI:
Axial images are best
Thickening of tendon sheath of first extensor compartment and diffuse irregular signal intensity in adjacent subcutaneous fat on T1 and T2
Stump Neuroma
Also called traumatic neuroma
Disorganised nonneoplastic proliferation of proximal end of severed/partially transected/injured nerve due to trauma or surgery
Usually painless, may be painful (especially on tapping/ palpation = Tinel sign))and may not respond to conservative therapy. Small, firm tender masses on palpation
Seen commonly in lower limbs, but also seen in oral cavity related to tooth extraction. Also seen in radial nerve and brachial plexus
Classification:
1. Spindle neuromas: Internal, focal, fusiform swellings, due to chronic friction or irritation to a nondisrupted, injured but intact nerve trunk
2. Terminal (lateral) neuromas: due to severe trauma with partial avulsion, disruption, or total transection of a nerve. Has a bulblous end. Usually after 1-12 months after amputation/trauma
Ultrasound:
Well defined, hypoechoic or similar to muscle
MRI:
Int on T1, int-to-high on T2 with ring like pattern (fascicular sign)
Treatment:
May be treated surgically or under ultrasound
Steroid is anti-inflammatory
Phenol produces severe demyelination and axonal degeneration
Glycerol works similarly, but is less effective
References:
1. Gruber H et al. Sonographically Guided Phenol Injection in Painful Stump Neuroma . AJR 2004; 182:952-954
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
Disorganised nonneoplastic proliferation of proximal end of severed/partially transected/injured nerve due to trauma or surgery
Usually painless, may be painful (especially on tapping/ palpation = Tinel sign))and may not respond to conservative therapy. Small, firm tender masses on palpation
Seen commonly in lower limbs, but also seen in oral cavity related to tooth extraction. Also seen in radial nerve and brachial plexus
Classification:
1. Spindle neuromas: Internal, focal, fusiform swellings, due to chronic friction or irritation to a nondisrupted, injured but intact nerve trunk
2. Terminal (lateral) neuromas: due to severe trauma with partial avulsion, disruption, or total transection of a nerve. Has a bulblous end. Usually after 1-12 months after amputation/trauma
Ultrasound:
Well defined, hypoechoic or similar to muscle
MRI:
Int on T1, int-to-high on T2 with ring like pattern (fascicular sign)
Treatment:
May be treated surgically or under ultrasound
Steroid is anti-inflammatory
Phenol produces severe demyelination and axonal degeneration
Glycerol works similarly, but is less effective
References:
1. Gruber H et al. Sonographically Guided Phenol Injection in Painful Stump Neuroma . AJR 2004; 182:952-954
2. Stuart RM et al. Sonography of Peripheral Nerve Pathology . AJR 2004; 182:123-129
SLAP lesions
Superior Labral AnteroPosterior Lesions (Synder 1990)
Tears are clasically located at biceps anchor
Begin posteriorly and extend anteriorly
Commonly occur at 12 O clock position
Superior labrum is loosely attached, more mobile and meniscal in appearance
Inferior labrum is firmly continuous with articular cartilage
Superior and anterosuperior labrum have diminished vascularity relative to the inferior labrum, hence more prone for degeneration
Superior portion of glenoid labrum serves as anchor for biceps tendon and provides stability
Impingement or rotator cuff tears can be caused by unstable biceps insertion, seen in SLAP lesions
Mechanism:
Compression force to shoulder, usually after fall onto an outstretched arm
traction on arm, due to sudden pull or repetitive overhead use, as in baseball pitchers, swimmers, tennis and volleyball players.
Clinical features:
Pain at the top of shoulder
Clicking, catchinganf pain on overhead activities
Anterior slide test
O'Brien test
Crank test
Classification & MR appearances:
Begin posteriorly and extend anteriorly, terminating before or at midglenoid notch
FS coronal oblique T1-weighted sequence provides highest sensitivity. Axials and sagittal help
SLAP I: degenerative fraying of free edge of superior glenoid labrum. High signal in superior labrum with irregular shape, stable biceps anchor. Non-surgical
SLAP II:most common type. Avulsion of labral–bicipital complex (superior labrum + biceps anchor) from superior glenoid. Detachment and inferior displacement of triangular superior labrum. Line of high signal across base of hyperintense labrum to periphery; biceps tendon shows normal signal and shape and attaches to the avulsed labrum. Gd tracks laterally
SLAP III: bucket-handle tears with preserved biceps anchor. line of high signal across base of hyperintense labrum extending beyond equator (undisplaced bucket-handle tear). Deficient superior labrum and the biceps tendon is followed to supraglenoid tubercle.
SLAP IV: bucket-handle tears with extension into biceps tendon. line of high signal across the base of normally hypointense labrum to periphery; extending beyond equator with deficient superior labrum + hyperintensity and splitting of the fibers of biceps tendon
SLAP V: anteroinferior Bankart lesion extending upward to include separation of the biceps tendon
SLAP VI: unstable radial or flap tears associated with separation of biceps anchor
SLAP VII: extension of SLAP lesion beneath middle glenohumeral ligament
False positives:
Sublabral foramen = sublabral hole = superior sublabral recess = Physiological detatchment of anterosuperior labrum. Located more anteriorly than SLAP lesion. Does not usually extend below the level of coracoid process. May be subdivided into 1. less than 2mm, 2. between 2-5mm and 3. more than 5mm. Extends medially (SLAP extends laterally) on coronal imaging. Tend to be better defined. Foramen is typically seen between 1-3 O clock postion
Meniscoid-type superior labrum - may be misinterpreted as type II SLAP lesion
Buford complex - deficient anterosuperior labrum with thickened or band like middle glenohumeral ligament. Can simulate detached anterior labrum
Ultrasound in Labral lesions:
Anterior labral tear:
Enlarged (more than 2mm) hypoechoic zone at base of labrum
Truncated shape or absence of labrum
Abnormal labral motility on dynamic scanning
References:
1. Waldt et al. Diagnostic Performance of MR Arthrography in the Assessment of Superior Labral Anteroposterior Lesions of the Shoulder . AJR 2004; 182:1271-1278
2. Bencardino JT et al. Superior Labrum Anterior- Posterior Lesions: Diagnosis with MR Arthrography of the Shoulder. Radiology. 2000;214:267-271
3. Connel DA et al. Noncontrast Magnetic Resonance Imaging of Superior Labral Lesions . The American Journal of Sports Medicine 27:208-213 (1999)
4. Robinson G et al. Normal anatomy and common labral lesions at MR arthrography of the shoulder. Clin Rad 61 (805-821)
Tears are clasically located at biceps anchor
Begin posteriorly and extend anteriorly
Commonly occur at 12 O clock position
Superior labrum is loosely attached, more mobile and meniscal in appearance
Inferior labrum is firmly continuous with articular cartilage
Superior and anterosuperior labrum have diminished vascularity relative to the inferior labrum, hence more prone for degeneration
Superior portion of glenoid labrum serves as anchor for biceps tendon and provides stability
Impingement or rotator cuff tears can be caused by unstable biceps insertion, seen in SLAP lesions
Mechanism:
Compression force to shoulder, usually after fall onto an outstretched arm
traction on arm, due to sudden pull or repetitive overhead use, as in baseball pitchers, swimmers, tennis and volleyball players.
Clinical features:
Pain at the top of shoulder
Clicking, catchinganf pain on overhead activities
Anterior slide test
O'Brien test
Crank test
Classification & MR appearances:
Begin posteriorly and extend anteriorly, terminating before or at midglenoid notch
FS coronal oblique T1-weighted sequence provides highest sensitivity. Axials and sagittal help
SLAP I: degenerative fraying of free edge of superior glenoid labrum. High signal in superior labrum with irregular shape, stable biceps anchor. Non-surgical
SLAP II:most common type. Avulsion of labral–bicipital complex (superior labrum + biceps anchor) from superior glenoid. Detachment and inferior displacement of triangular superior labrum. Line of high signal across base of hyperintense labrum to periphery; biceps tendon shows normal signal and shape and attaches to the avulsed labrum. Gd tracks laterally
SLAP III: bucket-handle tears with preserved biceps anchor. line of high signal across base of hyperintense labrum extending beyond equator (undisplaced bucket-handle tear). Deficient superior labrum and the biceps tendon is followed to supraglenoid tubercle.
SLAP IV: bucket-handle tears with extension into biceps tendon. line of high signal across the base of normally hypointense labrum to periphery; extending beyond equator with deficient superior labrum + hyperintensity and splitting of the fibers of biceps tendon
SLAP V: anteroinferior Bankart lesion extending upward to include separation of the biceps tendon
SLAP VI: unstable radial or flap tears associated with separation of biceps anchor
SLAP VII: extension of SLAP lesion beneath middle glenohumeral ligament
False positives:
Sublabral foramen = sublabral hole = superior sublabral recess = Physiological detatchment of anterosuperior labrum. Located more anteriorly than SLAP lesion. Does not usually extend below the level of coracoid process. May be subdivided into 1. less than 2mm, 2. between 2-5mm and 3. more than 5mm. Extends medially (SLAP extends laterally) on coronal imaging. Tend to be better defined. Foramen is typically seen between 1-3 O clock postion
Meniscoid-type superior labrum - may be misinterpreted as type II SLAP lesion
Buford complex - deficient anterosuperior labrum with thickened or band like middle glenohumeral ligament. Can simulate detached anterior labrum
Ultrasound in Labral lesions:
Anterior labral tear:
Enlarged (more than 2mm) hypoechoic zone at base of labrum
Truncated shape or absence of labrum
Abnormal labral motility on dynamic scanning
References:
1. Waldt et al. Diagnostic Performance of MR Arthrography in the Assessment of Superior Labral Anteroposterior Lesions of the Shoulder . AJR 2004; 182:1271-1278
2. Bencardino JT et al. Superior Labrum Anterior- Posterior Lesions: Diagnosis with MR Arthrography of the Shoulder. Radiology. 2000;214:267-271
3. Connel DA et al. Noncontrast Magnetic Resonance Imaging of Superior Labral Lesions . The American Journal of Sports Medicine 27:208-213 (1999)
4. Robinson G et al. Normal anatomy and common labral lesions at MR arthrography of the shoulder. Clin Rad 61 (805-821)
Posterior band IGHL lesions
POSTERIOR BAND OF IGHL LESIONS:
Far less common than anterior
Most are due to posterior dislocation
Posterior band is thinnest of inferior glenohumeral ligament
Injuries in posterior band of inferior glenohumeral ligament occur at glenoid (25%), mid substance (44%) and humerus (31%)
PHAGL lesion:
Posterior Humeral Avulsion of Glenohumeral Ligament
Humeral Avulsion of the Posterior Band of the Inferior Glenohumeral Ligament
Rare
References:
Chung CB et al. Humeral Avulsion of the Posterior Band of the Inferior Glenohumeral Ligament: MR Arthrography and Clinical Correlation in 17 Patients . AJR 2004; 183:355-359
Far less common than anterior
Most are due to posterior dislocation
Posterior band is thinnest of inferior glenohumeral ligament
Injuries in posterior band of inferior glenohumeral ligament occur at glenoid (25%), mid substance (44%) and humerus (31%)
PHAGL lesion:
Posterior Humeral Avulsion of Glenohumeral Ligament
Humeral Avulsion of the Posterior Band of the Inferior Glenohumeral Ligament
Rare
References:
Chung CB et al. Humeral Avulsion of the Posterior Band of the Inferior Glenohumeral Ligament: MR Arthrography and Clinical Correlation in 17 Patients . AJR 2004; 183:355-359
GCT of tendon sheath
Introduction:
Also known as localized nodular tenosynovitis
Most often on the volar aspect (flexor tendon) of fingers, close to distal joints
Pathologically identical to PVNS
In close contact with tendon
Can cause bone erosions
Malignant changes are rare
Clinical features:
Soft-tissue swelling and pain
Treatment and prognosis:
Surgery. But radical excision with negative margin is not indicated
Recurrence 10% to 20%
Ultrasound:
Uniformly hypoechoic, may be heterogenous. Posterior enhancement is not common
In contact/ close relation with a tendon or evn may be encased. But usually does not move with tendon, because the tumor arises from sheath, not from tendon itself
usually no cystic component/ hyperechogenicity/ calcification
Bone erosions may be diagnosed
Vascular on Doppler
Differential: ganglion - usually cystic, unless ruptured
References:
Middleton WD et al. Giant Cell Tumors of the Tendon Sheath: Analysis of Sonographic Findings. AJR 2004; 183:337-339
Also known as localized nodular tenosynovitis
Most often on the volar aspect (flexor tendon) of fingers, close to distal joints
Pathologically identical to PVNS
In close contact with tendon
Can cause bone erosions
Malignant changes are rare
Clinical features:
Soft-tissue swelling and pain
Treatment and prognosis:
Surgery. But radical excision with negative margin is not indicated
Recurrence 10% to 20%
Ultrasound:
Uniformly hypoechoic, may be heterogenous. Posterior enhancement is not common
In contact/ close relation with a tendon or evn may be encased. But usually does not move with tendon, because the tumor arises from sheath, not from tendon itself
usually no cystic component/ hyperechogenicity/ calcification
Bone erosions may be diagnosed
Vascular on Doppler
Differential: ganglion - usually cystic, unless ruptured
References:
Middleton WD et al. Giant Cell Tumors of the Tendon Sheath: Analysis of Sonographic Findings. AJR 2004; 183:337-339
Isolated greater trochonter fracture
Rare
Most common site is tip and upper portion in adults. Actually more complex than what they appear on plain radiographs. MRI is useful to further characterise.
References:
Feldman F et al. MRI of Seemingly Isolated Greater Trochanteric Fractures . AJR 2004; 183:323-329
Image gallery:
Plain film:

CT correlation:
Most common site is tip and upper portion in adults. Actually more complex than what they appear on plain radiographs. MRI is useful to further characterise.
References:
Feldman F et al. MRI of Seemingly Isolated Greater Trochanteric Fractures . AJR 2004; 183:323-329
Image gallery:
Plain film:
CT correlation:
Fractures & Dislocations
FRACTURE TYPES:
Avulsion injuries
Stress fracture (fatigue fracture)
Tibial stress fracture
Fibular stress fracture
Calcaneal stress fracture
March fracture
Insufficiency fracture:
Para-acetabular insufficiency fracture
Pathological fracture:
Occult fractures: Occult fractures
NAI:
Bucket Handle fracture = Corner fracture
Paediatic fractures:
Epiphyseal injuries
Torus fracture = Buckle fracture Bowing fracture
Green stick fracture
Toddler's fracture = spiral hairline fracture of mid tibia
Little League elbow
Nursemaid elbow = long axis of radius may not intersect capitellum on AP and lateral views
Wagon wheel fracture = distal femoral epiphysis from the main portion of the femur in a child
FRACTURES - REGIONWISE
Skull:
Linear fracture
Depressed fracture
Petrous temporal fracture
Face and Mandible:
Tripod fracture
Isolated zygomatic arch fracture
Fracture alveolar process of maxilla
Blow out fracture of orbit
LeFort fractures
Fracture mandible
Cervical spine:
Atlas fractures
Axis fractures
C3-C7 fractures
Thoracic spine:
Burst fracture
Chance fracture = Seat belt fracture
Lumbar spine:
Compression fractures
Porotic fractures
Dashboard fracture
Jumper fracture
Pelvis and Sacrum:
Duverney fracture = fracture iliac wing
Malgaigne fracture
Pelvis
Acetabulum:
Acetabular fractures
Para-acetabular insufficiency fracture
Sacrum:
Sacral fractures
Jumper fracture = Transverse fracture of upper sacrum (suicidal attempt)
Thorax:
Sternal fracture
Rib fractures
Sternoclavicular joint injury
Clavicle and scapula:
Clavicle fracture
Scapular fracture
Shoulder joint and Arm:
Hill Sachs lesion
Bankart lesion
Elbow and Forearm:
Radial head fracture
Diaphyseal Fractures of forearm
Essex-Lopresti injury
Galeazzi Fractures and Dislocations
Monteggia Fracture-Dislocations
Chisel fracture = Incomplete radial head fracture
Panners disease = fragmentation of capitellum
Nightstick fracture = Parry fracture = isolated ulnar shaft fracture
Nursemaid elbow
Wrist and Hand:
Carpal injuries
Colles fracture
Smith fracture
Barton fracture
Chauffeur fracture = Backfire fracture = Lorry driver fracture = Hutchison fracture = Radial styloid fracture with radiocarpal joint extension
Scaphoid fracture
Kienbocks fracture
Triquetral fracture
Scapholunate dislocation
Hook of Hamate fracture = Golfer wrist (non-dominant hand)
Locked metacarpophalyngeal joint
Dislocation of 5th CMCJ
Boxer fracture = Brawler fracture = fracture neck of 4/5th metacarpal
Bennett fracture
Rolando fracture
Gamekeeper's thumb = Skier pole thumb = Skier thumb = Break dancer thumb = Base of PP of thumb
Jersey Finger = Avulsion fracture of base of distal phalanx of a finger, most common is ring finger (common in American football players)
Mallet finger = Baseball finger = Dropped finger
Hip joint and Thigh:
Dashboard fracture = Posterior rim of acetabelum fracture
Fracture neck of the femur
Isolated greater trochanter fracture
Isolated lesser trochanter fracture = patholgical unless proved otherwise
Periprosthetic hip fracture
Knee and Leg:
Patellar fractures
Tibial plateau fracture
Fibular stress fracture
Wagon wheel fracture = distal femoral epiphysis from the main portion of the femur in a child
Bumper fracture = Cotton fracture
Pellagrini Stieda lesion
Segond fracture
Tibial stress fracture
Ankle and foot:
Calcaneal fractures
Runner fracture = Stress fracture of distal fibula 2 inches above lateral malleolus
Lover's fracture = calcaneal fracture due to fall from height
Calcaneal fractures
Calcaneal stress fracture
Snowboarder fracture = fracture lateral process of talus
Cuboid dislocation
Lisfranc fracture dislocation
Fracture base of 5th metatarsal = Dancer's fracture
Jones' fracture = Fracture base of 5th metatarsal distal to tuberosity
March fracture = stress fracture of one of the metatarsals
Frieberg's lesion
Avulsion injuries
Stress fracture (fatigue fracture)
Tibial stress fracture
Fibular stress fracture
Calcaneal stress fracture
March fracture
Insufficiency fracture:
Para-acetabular insufficiency fracture
Pathological fracture:
Occult fractures: Occult fractures
NAI:
Bucket Handle fracture = Corner fracture
Paediatic fractures:
Epiphyseal injuries
Torus fracture = Buckle fracture Bowing fracture
Green stick fracture
Toddler's fracture = spiral hairline fracture of mid tibia
Little League elbow
Nursemaid elbow = long axis of radius may not intersect capitellum on AP and lateral views
Wagon wheel fracture = distal femoral epiphysis from the main portion of the femur in a child
FRACTURES - REGIONWISE
Skull:
Linear fracture
Depressed fracture
Petrous temporal fracture
Face and Mandible:
Tripod fracture
Isolated zygomatic arch fracture
Fracture alveolar process of maxilla
Blow out fracture of orbit
LeFort fractures
Fracture mandible
Cervical spine:
Atlas fractures
Axis fractures
C3-C7 fractures
Thoracic spine:
Burst fracture
Chance fracture = Seat belt fracture
Lumbar spine:
Compression fractures
Porotic fractures
Dashboard fracture
Jumper fracture
Pelvis and Sacrum:
Duverney fracture = fracture iliac wing
Malgaigne fracture
Pelvis
Acetabulum:
Acetabular fractures
Para-acetabular insufficiency fracture
Sacrum:
Sacral fractures
Jumper fracture = Transverse fracture of upper sacrum (suicidal attempt)
Thorax:
Sternal fracture
Rib fractures
Sternoclavicular joint injury
Clavicle and scapula:
Clavicle fracture
Scapular fracture
Shoulder joint and Arm:
Hill Sachs lesion
Bankart lesion
Elbow and Forearm:
Radial head fracture
Diaphyseal Fractures of forearm
Essex-Lopresti injury
Galeazzi Fractures and Dislocations
Monteggia Fracture-Dislocations
Chisel fracture = Incomplete radial head fracture
Panners disease = fragmentation of capitellum
Nightstick fracture = Parry fracture = isolated ulnar shaft fracture
Nursemaid elbow
Wrist and Hand:
Carpal injuries
Colles fracture
Smith fracture
Barton fracture
Chauffeur fracture = Backfire fracture = Lorry driver fracture = Hutchison fracture = Radial styloid fracture with radiocarpal joint extension
Scaphoid fracture
Kienbocks fracture
Triquetral fracture
Scapholunate dislocation
Hook of Hamate fracture = Golfer wrist (non-dominant hand)
Locked metacarpophalyngeal joint
Dislocation of 5th CMCJ
Boxer fracture = Brawler fracture = fracture neck of 4/5th metacarpal
Bennett fracture
Rolando fracture
Gamekeeper's thumb = Skier pole thumb = Skier thumb = Break dancer thumb = Base of PP of thumb
Jersey Finger = Avulsion fracture of base of distal phalanx of a finger, most common is ring finger (common in American football players)
Mallet finger = Baseball finger = Dropped finger
Hip joint and Thigh:
Dashboard fracture = Posterior rim of acetabelum fracture
Fracture neck of the femur
Isolated greater trochanter fracture
Isolated lesser trochanter fracture = patholgical unless proved otherwise
Periprosthetic hip fracture
Knee and Leg:
Patellar fractures
Tibial plateau fracture
Fibular stress fracture
Wagon wheel fracture = distal femoral epiphysis from the main portion of the femur in a child
Bumper fracture = Cotton fracture
Pellagrini Stieda lesion
Segond fracture
Tibial stress fracture
Ankle and foot:
Calcaneal fractures
Runner fracture = Stress fracture of distal fibula 2 inches above lateral malleolus
Lover's fracture = calcaneal fracture due to fall from height
Calcaneal fractures
Calcaneal stress fracture
Snowboarder fracture = fracture lateral process of talus
Cuboid dislocation
Lisfranc fracture dislocation
Fracture base of 5th metatarsal = Dancer's fracture
Jones' fracture = Fracture base of 5th metatarsal distal to tuberosity
March fracture = stress fracture of one of the metatarsals
Frieberg's lesion
wrist and hand
Anatomy:
TFCC anatomy
Measurements in wrist
Bone:
Ulnar variance
TFCC:
TFCC anatomy
TFCC injury
Nerve:
Carpal tunnel syndrome
Tendons:
Imaging extensor tendons of the wrist
de Quervain's tenosynovitis
Intersection syndrome
Imaging flexor tendons of the wrist
Ligaments:
Radial collateral ligament injuries of thumb
Impaction/ impingement/ abutment syndromes:
Ulnar sided impaction syndromes
Degenerative :
SLAC (ScapohoLunate Advanced Collapse)
Tumor and tumor like conditions:
Neural fibrolipoma
Trauma:
Imaging in trauma
Carpal injuries
Locked metacarpophalyngeal joint
fracture non-union and AVN scaphoid
Arthrography:
CT wrist arthrogram
First MCPJ:
Imaging UCL of 1st MCPJ
TFCC anatomy
Measurements in wrist
Bone:
Ulnar variance
TFCC:
TFCC anatomy
TFCC injury
Nerve:
Carpal tunnel syndrome
Tendons:
Imaging extensor tendons of the wrist
de Quervain's tenosynovitis
Intersection syndrome
Imaging flexor tendons of the wrist
Ligaments:
Radial collateral ligament injuries of thumb
Impaction/ impingement/ abutment syndromes:
Ulnar sided impaction syndromes
Degenerative :
SLAC (ScapohoLunate Advanced Collapse)
Tumor and tumor like conditions:
Neural fibrolipoma
Trauma:
Imaging in trauma
Carpal injuries
Locked metacarpophalyngeal joint
fracture non-union and AVN scaphoid
Arthrography:
CT wrist arthrogram
First MCPJ:
Imaging UCL of 1st MCPJ
carpal tunnel syndrome
Introduction:
Diagnosis is based on combination of symptoms and electrophysiologic tests
Anatomy:
Anatomical space bounded anteriorly by flexor retinaculum and posteriorly by 8 carpal bones
Contents: median nerve and flexor tendons
(Median nerve has sensory supply to radial 3 1/2 fingers and motor supply to short abductor and opposing muscles of thumb, radial half of short flexors of thumb, and two lateral lumbricals)
Clinical features:
Sensory: Tingling and numbness of lateral 3 1/2 digits, nocturnal pain
Motor: Weakness of thumb, thenar atrophy
Autonomic: anhidrosis due to compression of median nerve
Phalen maneuver: tingling of fingers upon flexing the wrist for 60 seconds.
Tinel sign: tingling of fingers upon tapping median nerve at wrist
Causes:
Most are idiopathic
Others: Repetitive stress injury, RA, acromegaly, myxedema, pregnancy, oral contraceptives, acute or chronic trauma, amyloidosis
Rare: sarcoidosis, tuberculosis, Paget disease, vascular shunts
Extremely rare: anomalous superficial flexor muscle of fingers, anomalous lumbrical muscles, thrombosis of persistent median artery, bleeding dyscrasia, fibroma of tendon sheath, ganglion cyst, lipoma, lipofibromatous hamartoma of median nerve, osteochondroma leading to carpal tunnel syndrome
Electrophysiology:
Difference of more than 0.4 ms between the median and ulnar sensory peak latencies or a prolonged median distal motor latency of more than 4 msec
Ultrasound:
13MHz linear probe
Arms extended, forearms were supinated, wrists rested on flat surface, fingers semiextended
Transverse images of median nerve immediately proximal to the carpal tunnel inlet, at carpal tunnel inlet and at carpal tunnel outlet
Flexor retinaculum, seen as arched echogenic band, is used as landmark for the carpal tunnel, not bones and is seen anterior to the median nerve
Median nerve is seen superficial to the flexor tendons, seen as oval shaped well defined ehogenic structure with speckeled appearance proximal to the carpal tunnel and loses speckeled appearance distally and becomes less well defined
Cutoff of 0.09 - 0.11 sq.cm may be taken as cut-off
MRI:
Thickening of the median nerve
Flattening of the median nerve
Palmar bowing of the flexor retinaculum
References:
Wong SM et al. Carpal Tunnel Syndrome: Diagnostic Usefulness of Sonography. Radiology 2004;232:93-99
K Monagle K et al. Quantitative MR imaging of carpal tunnel syndrome. AJR Jun 1999; 172: 1581 - 1586.
Mallouhi A et al. Predictors of Carpal Tunnel Syndrome: Accuracy of Gray-Scale and Color Doppler Sonography. AJR May 2006; 186: 1240 - 1245
Diagnosis is based on combination of symptoms and electrophysiologic tests
Anatomy:
Anatomical space bounded anteriorly by flexor retinaculum and posteriorly by 8 carpal bones
Contents: median nerve and flexor tendons
(Median nerve has sensory supply to radial 3 1/2 fingers and motor supply to short abductor and opposing muscles of thumb, radial half of short flexors of thumb, and two lateral lumbricals)
Clinical features:
Sensory: Tingling and numbness of lateral 3 1/2 digits, nocturnal pain
Motor: Weakness of thumb, thenar atrophy
Autonomic: anhidrosis due to compression of median nerve
Phalen maneuver: tingling of fingers upon flexing the wrist for 60 seconds.
Tinel sign: tingling of fingers upon tapping median nerve at wrist
Causes:
Most are idiopathic
Others: Repetitive stress injury, RA, acromegaly, myxedema, pregnancy, oral contraceptives, acute or chronic trauma, amyloidosis
Rare: sarcoidosis, tuberculosis, Paget disease, vascular shunts
Extremely rare: anomalous superficial flexor muscle of fingers, anomalous lumbrical muscles, thrombosis of persistent median artery, bleeding dyscrasia, fibroma of tendon sheath, ganglion cyst, lipoma, lipofibromatous hamartoma of median nerve, osteochondroma leading to carpal tunnel syndrome
Electrophysiology:
Difference of more than 0.4 ms between the median and ulnar sensory peak latencies or a prolonged median distal motor latency of more than 4 msec
Ultrasound:
13MHz linear probe
Arms extended, forearms were supinated, wrists rested on flat surface, fingers semiextended
Transverse images of median nerve immediately proximal to the carpal tunnel inlet, at carpal tunnel inlet and at carpal tunnel outlet
Flexor retinaculum, seen as arched echogenic band, is used as landmark for the carpal tunnel, not bones and is seen anterior to the median nerve
Median nerve is seen superficial to the flexor tendons, seen as oval shaped well defined ehogenic structure with speckeled appearance proximal to the carpal tunnel and loses speckeled appearance distally and becomes less well defined
Cutoff of 0.09 - 0.11 sq.cm may be taken as cut-off
MRI:
Thickening of the median nerve
Flattening of the median nerve
Palmar bowing of the flexor retinaculum
References:
Wong SM et al. Carpal Tunnel Syndrome: Diagnostic Usefulness of Sonography. Radiology 2004;232:93-99
K Monagle K et al. Quantitative MR imaging of carpal tunnel syndrome. AJR Jun 1999; 172: 1581 - 1586.
Mallouhi A et al. Predictors of Carpal Tunnel Syndrome: Accuracy of Gray-Scale and Color Doppler Sonography. AJR May 2006; 186: 1240 - 1245
Spine
Anatomy:
Lumbar facet joints
Differentials:
Differentiating benign and malignant spinal compression fractures
Fractures:
Compression fractures
Atlas fractures
Axis fractures
C3-C7 fractures
Chance fracture
Compression fractures
Para-acetabular insufficiency fracture
Marrow:
Spinal bone marrow
Tumour and tumor like conditions:
Spinal tumours
Cervical spine:
Atlas fractures
Axis fractures
C3-C7 fractures
Thoracolumbar spine:
Chance fracture
Lumbar spine:
Evaluation of back pain
Approach to LS spine MRI
Compression fractures
Degenerative disease of lumbar spine
Disc herniation
Acetabulum:
Para-acetabular insufficiency fracture
Symphysis pubis:
Secondary cleft sign
Miscellaneous:
Pyriformis syndrome
Baastrups's disease
Lumbar facet joints
Differentials:
Differentiating benign and malignant spinal compression fractures
Fractures:
Compression fractures
Atlas fractures
Axis fractures
C3-C7 fractures
Chance fracture
Compression fractures
Para-acetabular insufficiency fracture
Marrow:
Spinal bone marrow
Tumour and tumor like conditions:
Spinal tumours
Cervical spine:
Atlas fractures
Axis fractures
C3-C7 fractures
Thoracolumbar spine:
Chance fracture
Lumbar spine:
Evaluation of back pain
Approach to LS spine MRI
Compression fractures
Degenerative disease of lumbar spine
Disc herniation
Acetabulum:
Para-acetabular insufficiency fracture
Symphysis pubis:
Secondary cleft sign
Miscellaneous:
Pyriformis syndrome
Baastrups's disease
Hip
Journal reviews
Anatomy:
Hip joint
Acetabular labrum
Hamstring mucle complex
Clinical:
Causes of hip pain
Causes of groin pain (sports)
Abdominal wall:
Ultrsaound of hernias
Joint:
Osteoarthritis of the hip joint
Hip in rheumatoid disorders
Femoroacetabular impingement
Imaging acetabular labrum
Labrum:
Anatomy
Imaging labrum
Femoral head:
AVN
Muscle:
Hamstring muscle complex injuries
Pyriformis syndrome
Hip abductor tendon tears
Imaging iliopsoas
Sports hernia
THR:
THR radiographic appearances
THR loosening
THR infection
Aggresive granumomatous disease
Heterotopic bone formation
Greater tuberosity and gluteals:
Trochanteric bursitis (greater tuberosity pain syndrome)
Common tumors:
Intertrochontric region - Intraosseus lipoma, Liposclerosing myxofibrous tumor of bone
Interventions:
iliopsoas bursal injection
Lateral cutaneous nerve of thigh
Anatomy:
Hip joint
Acetabular labrum
Hamstring mucle complex
Clinical:
Causes of hip pain
Causes of groin pain (sports)
Abdominal wall:
Ultrsaound of hernias
Joint:
Osteoarthritis of the hip joint
Hip in rheumatoid disorders
Femoroacetabular impingement
Imaging acetabular labrum
Labrum:
Anatomy
Imaging labrum
Femoral head:
AVN
Muscle:
Hamstring muscle complex injuries
Pyriformis syndrome
Hip abductor tendon tears
Imaging iliopsoas
Sports hernia
THR:
THR radiographic appearances
THR loosening
THR infection
Aggresive granumomatous disease
Heterotopic bone formation
Greater tuberosity and gluteals:
Trochanteric bursitis (greater tuberosity pain syndrome)
Common tumors:
Intertrochontric region - Intraosseus lipoma, Liposclerosing myxofibrous tumor of bone
Interventions:
iliopsoas bursal injection
Lateral cutaneous nerve of thigh
pyriformis syndrome
Etiology:
Rare entrapment neuropathy, causing lower back pain and sciatica, due to sciatic nerve entrapment at greater sciatic notch
Usually due piriformis hypertrophy; other causes include inflammation, anatomic variations, trauma, pseudoaneurysm of inferior gluteal artery, excessive exercise, inflammation and spasm of piriformis muscle, infection
Clinical features:
Frequently delay in the diagnosis or misdiagnosed
Usually diagnosis of exclusion
6% of lower back pain and sciatica may be caused by piriformis syndrome
Pain and paresthesias in the unilateral gluteal region radiating to the hip and posterior thigh in a sciatic radicular distribution
Symptoms can be reproduced by digital pressure over the belly of the piriformis muscle in the gluteal region and on the lateral pelvic wall of the affected side
Freiberg sign - pain with forced internal rotation of extended thigh
Sign of Pace and Nagle - pain with resistance to abduction and external rotation of thigh
Imaging:
MR is investigation of choic although CT may be useful
Hypertrophy of pyriformis the most common finding
Bone scan may show abnormal uptake in the soft tissue
Treatment:
Treat the cause, usually surgically
Local injection is possible
References:
Lee EY et al. MRI of pyriformis syndrome. AJR 2004; 183:63-64
Beauchesne RP et al.Myositis Ossificans of the Piriformis Muscle: An Unusual Cause of Piriformis Syndrome: A Case Report. The Journal of Bone and Joint Surgery 79:906-10 (1997)
Rare entrapment neuropathy, causing lower back pain and sciatica, due to sciatic nerve entrapment at greater sciatic notch
Usually due piriformis hypertrophy; other causes include inflammation, anatomic variations, trauma, pseudoaneurysm of inferior gluteal artery, excessive exercise, inflammation and spasm of piriformis muscle, infection
Clinical features:
Frequently delay in the diagnosis or misdiagnosed
Usually diagnosis of exclusion
6% of lower back pain and sciatica may be caused by piriformis syndrome
Pain and paresthesias in the unilateral gluteal region radiating to the hip and posterior thigh in a sciatic radicular distribution
Symptoms can be reproduced by digital pressure over the belly of the piriformis muscle in the gluteal region and on the lateral pelvic wall of the affected side
Freiberg sign - pain with forced internal rotation of extended thigh
Sign of Pace and Nagle - pain with resistance to abduction and external rotation of thigh
Imaging:
MR is investigation of choic although CT may be useful
Hypertrophy of pyriformis the most common finding
Bone scan may show abnormal uptake in the soft tissue
Treatment:
Treat the cause, usually surgically
Local injection is possible
References:
Lee EY et al. MRI of pyriformis syndrome. AJR 2004; 183:63-64
Beauchesne RP et al.Myositis Ossificans of the Piriformis Muscle: An Unusual Cause of Piriformis Syndrome: A Case Report. The Journal of Bone and Joint Surgery 79:906-10 (1997)
cubital bursitis (bicepitoradial bursitis)
Also known as bicepitoradial bursitis
Rare painful condition of elbow
Anatomy:
2 bursae in the anterior elbow joint.
1. Bicipitoradial (cubital) bursa: Cubital bursa is seen between distal biceps tendon and anterior part of radial tuberosity, tracks along medial cortex of radius and wraps around distal biceps tendon. The biceps tendon inserts into the rough posterior area of the bicipital tuberosity, and bicepitoradial bursa separates it from the smooth anterior area of the tuberosity. Compressed in pronation Usually not seen on US or MR
2. Interosseous medial bursa: present in 20%, adjacent to biceps along the brachialis; may compress median nerve
Both may communicate with each other
Etiology:
Due due repitative supination and pronation mechanical injury
Trauma, RA, CPPD, PVNS, infection, synovial chondromatosis, chemical synovitis, bone proliferation/spur
Associated with tear
Clinical features:
Painful swelling in the antecubital fossa, loss of motion, locking
Crepitation, palpable loose bodies
Can cause compression on the median or posterior interosseous nerve
Ultrasound:
7.5-12 MHz
Power Doppler assesses the degree of inflammation
Bursitis is seen as anechoic/ hypoechoic lesion with/without echogenic debris/ calcifications wrapping the biceps tendon and superficial to it
Distal biceps tendon is usually intact
Can be treated with ultrasound guided aspiration (22G) and injecting 2 mL of 1% lignocaine (25%); 0.5% bupivacaine (25%) and triamcinolone (40 mg/mL) (Kenalogis) (50%) is injected
MRI:
Better anatomical details
References:
1. Sofka CM et al. Sonography of cubital bursitis. AJR 2004; 183:51-53
2. Matsumoto K et al. Cubital Bursitis Caused by Localized Synovial Chondromatosis of the Elbow. A Case Report. The Journal of Bone and Joint Surgery 78:275-7 (1996)
3. Chew ML et al. Disorders of the Distal Biceps Brachii Tendon. RadioGraphics 2005;25:1227-1237
Rare painful condition of elbow
Anatomy:
2 bursae in the anterior elbow joint.
1. Bicipitoradial (cubital) bursa: Cubital bursa is seen between distal biceps tendon and anterior part of radial tuberosity, tracks along medial cortex of radius and wraps around distal biceps tendon. The biceps tendon inserts into the rough posterior area of the bicipital tuberosity, and bicepitoradial bursa separates it from the smooth anterior area of the tuberosity. Compressed in pronation Usually not seen on US or MR
2. Interosseous medial bursa: present in 20%, adjacent to biceps along the brachialis; may compress median nerve
Both may communicate with each other
Etiology:
Due due repitative supination and pronation mechanical injury
Trauma, RA, CPPD, PVNS, infection, synovial chondromatosis, chemical synovitis, bone proliferation/spur
Associated with tear
Clinical features:
Painful swelling in the antecubital fossa, loss of motion, locking
Crepitation, palpable loose bodies
Can cause compression on the median or posterior interosseous nerve
Ultrasound:
7.5-12 MHz
Power Doppler assesses the degree of inflammation
Bursitis is seen as anechoic/ hypoechoic lesion with/without echogenic debris/ calcifications wrapping the biceps tendon and superficial to it
Distal biceps tendon is usually intact
Can be treated with ultrasound guided aspiration (22G) and injecting 2 mL of 1% lignocaine (25%); 0.5% bupivacaine (25%) and triamcinolone (40 mg/mL) (Kenalogis) (50%) is injected
MRI:
Better anatomical details
References:
1. Sofka CM et al. Sonography of cubital bursitis. AJR 2004; 183:51-53
2. Matsumoto K et al. Cubital Bursitis Caused by Localized Synovial Chondromatosis of the Elbow. A Case Report. The Journal of Bone and Joint Surgery 78:275-7 (1996)
3. Chew ML et al. Disorders of the Distal Biceps Brachii Tendon. RadioGraphics 2005;25:1227-1237
glenohumoral joint arthorgraphy
Oberholzer (1933)
Indications:
Diagnostic arthrography is nearly obsolete
Diagnostic for MR arhrogram
Therapeutic for adhesive capsulitis with distention arthrography, steroids, radioactive synovectomy
Palpation directed arthrography:
Not a popular technique, but has been used (3)
AP (Schneider) technique:(1975)
Straight AP approach with 3.5-inch 22Gneedle directed vertically at junction of middle and lower thirds of glenohumeral joint under fluoroscopy
Pitfall - distortion of inferior GHL and anteroinferior labrum, thus creating confounding findings on MR arthrogram
Modified AP technique (rotator cuff interval):
Spares subscapularis, inferior GHL, anteroinferior labrum and long head of biceps
Arm in external rotation (palm up)
Mark the skin over upper medial quadrant of humeral head close to articular joint line with X-ray tube perpendicular to table
Advance the needle (1.5 inch 22 G) parallel to X-ray beam or with slight medial angulation until in contact with humeral head.
Low resistance 0.5–1.0 mL of anesthetic helps to ascertain intraarticular position
Then inject the required contrast
Posterior approach:
Arm midway between supination and pronation, i.e., shoulder in neutral position
Pad under patient's torso to raise the side
Glenohumeral joint to be seen tangentially
Skin marked over inferomedial quadrant of humeral head
21G needle
Ultrasound guided arthrography:
Semiprone with affected shoulder uppermost
Ipsilateral arm placed over pillow to maintain semiprone position
Anterior approach may also be used
5-12MHz linear probe
Probe along the long axis of musculotendinous junction of infraspinatus, just inferior to the scapular spine, with posterior glenoid rim and posterior glenohumeral joint line centered in the field of view with clear view of the contours of the posterior glenoid rim, posterior glenoid labrum and humeral head.
Humeral head seen as curved echogenic line, posterior glenoid rim as triangular echogenic structure, posterior glenoid labrum as homogenously echogenic triangular structure
20- to 22-gauge spinal needle through infraspinatus tendon, then feeling of capsular resistance followed by resistance-free space
Injection into the joint without any resistance
No fluid distention is seen on ultrasound at posterior glenohumeral joint recess because the injected substance runs freely into anterior joint recess which is not seen. If fluid is seen pooling around the needle tip, it means the needle tip is not in the right place
If a large volume is instilled, the posterior recess also distends
Contrast:
0.1-0.2 mL of Gd in 20 mL of saline
Inject up to 12-20 mL
References:
1. Dépelteau H et al. Arthrography of the Shoulder: A Simple Fluoroscopically Guided Approach for Targeting the Rotator Cuff Interval . AJR 2004; 182:329-332
2. Zwar RB et al. Sonographically Guided Glenohumeral Joint Injection. AJR 2004; 183:48-50
Valls R et al. Sonographic guidance of needle position for MR arthrography of the shoulder. AJR1997; 169:845 –847
3. DeMouy EH et al. Palpation-directed (non–fluoroscopically guided) saline-enhanced MR arthrography of the shoulder. AJR1997; 169:229 –231
4. Farmer KD et al. MR Arthrography of the Shoulder: Fluoroscopically Guided Technique Using a Posterior Approach. AJR 2002; 178:433-434
Indications:
Diagnostic arthrography is nearly obsolete
Diagnostic for MR arhrogram
Therapeutic for adhesive capsulitis with distention arthrography, steroids, radioactive synovectomy
Palpation directed arthrography:
Not a popular technique, but has been used (3)
AP (Schneider) technique:(1975)
Straight AP approach with 3.5-inch 22Gneedle directed vertically at junction of middle and lower thirds of glenohumeral joint under fluoroscopy
Pitfall - distortion of inferior GHL and anteroinferior labrum, thus creating confounding findings on MR arthrogram
Modified AP technique (rotator cuff interval):
Spares subscapularis, inferior GHL, anteroinferior labrum and long head of biceps
Arm in external rotation (palm up)
Mark the skin over upper medial quadrant of humeral head close to articular joint line with X-ray tube perpendicular to table
Advance the needle (1.5 inch 22 G) parallel to X-ray beam or with slight medial angulation until in contact with humeral head.
Low resistance 0.5–1.0 mL of anesthetic helps to ascertain intraarticular position
Then inject the required contrast
Posterior approach:
Arm midway between supination and pronation, i.e., shoulder in neutral position
Pad under patient's torso to raise the side
Glenohumeral joint to be seen tangentially
Skin marked over inferomedial quadrant of humeral head
21G needle
Ultrasound guided arthrography:
Semiprone with affected shoulder uppermost
Ipsilateral arm placed over pillow to maintain semiprone position
Anterior approach may also be used
5-12MHz linear probe
Probe along the long axis of musculotendinous junction of infraspinatus, just inferior to the scapular spine, with posterior glenoid rim and posterior glenohumeral joint line centered in the field of view with clear view of the contours of the posterior glenoid rim, posterior glenoid labrum and humeral head.
Humeral head seen as curved echogenic line, posterior glenoid rim as triangular echogenic structure, posterior glenoid labrum as homogenously echogenic triangular structure
20- to 22-gauge spinal needle through infraspinatus tendon, then feeling of capsular resistance followed by resistance-free space
Injection into the joint without any resistance
No fluid distention is seen on ultrasound at posterior glenohumeral joint recess because the injected substance runs freely into anterior joint recess which is not seen. If fluid is seen pooling around the needle tip, it means the needle tip is not in the right place
If a large volume is instilled, the posterior recess also distends
Contrast:
0.1-0.2 mL of Gd in 20 mL of saline
Inject up to 12-20 mL
References:
1. Dépelteau H et al. Arthrography of the Shoulder: A Simple Fluoroscopically Guided Approach for Targeting the Rotator Cuff Interval . AJR 2004; 182:329-332
2. Zwar RB et al. Sonographically Guided Glenohumeral Joint Injection. AJR 2004; 183:48-50
Valls R et al. Sonographic guidance of needle position for MR arthrography of the shoulder. AJR1997; 169:845 –847
3. DeMouy EH et al. Palpation-directed (non–fluoroscopically guided) saline-enhanced MR arthrography of the shoulder. AJR1997; 169:229 –231
4. Farmer KD et al. MR Arthrography of the Shoulder: Fluoroscopically Guided Technique Using a Posterior Approach. AJR 2002; 178:433-434
Elbow
ELBOW AND FOREARM:
Anatomy:
Muscles of elbow
Ligaments:
Imaging ulnar collateral ligament
Imaging lateral collateral ligament complex
Annular ligament
Imaging Annular Ligament of the elbow
Tendons and Muscles:
Distal biceps tendon injuries
Medial epicondylitis
Bursae:
Olecranon bursitis
Cubital (bicepitoradial) bursitis
Osteochondral injuries:
Osteochondritis Dissecans of the Capitellum
Syndromes:
Cubital tunnel syndrome (ulnar N)
Radial tunnel syndrome (posterior interossous N)
Anatomy:
Muscles of elbow
Ligaments:
Imaging ulnar collateral ligament
Imaging lateral collateral ligament complex
Annular ligament
Imaging Annular Ligament of the elbow
Tendons and Muscles:
Distal biceps tendon injuries
Medial epicondylitis
Bursae:
Olecranon bursitis
Cubital (bicepitoradial) bursitis
Osteochondral injuries:
Osteochondritis Dissecans of the Capitellum
Syndromes:
Cubital tunnel syndrome (ulnar N)
Radial tunnel syndrome (posterior interossous N)
Olecranon bursitis
Synonyms:
Student's elbow, Miner's elbow
Anatomy:
Several bursa occur in the posterior aspect of the elbow. Three common bursa occur and they include olecranon bursa (subcutaneous posterior to olecranon), deep intratendinoud bursa (within triceps near its insertion), deep subtendinous bursa (deep to triceps near insertion). Other uncommon bursae are subcutaneous medial and lateral epicondylar bursa, ulnar nerve bursa, subanconeous bursa.
Etiology:
Non-septic (2/3) : overuse, repeated traumatization (students, miners, American footballers), inflammatory arthropathy, obesity, uremia, RA, gout,
Septic (1/3): S.Auerus in 90%, rest in beta-hemolytic streptococcus. Riska include alcohol abuse, steroids, diabetes, renal impairment, malignancy
Clinical features:
Olecranon bursitis is a clinical diagnosis, and MRI is rarely performed. Clinical differentiation of septic and nonseptic bursitis may be difficult.
MRI:
Olecranon bursitis is a clinical diagnosis, and MRI is rarely performed. On Gd, rim enhancement is seen, even in non-septic bursitis. Associated features include joint effusion, soft tissue edema, thickened tricpes, bone marrow edema. It is not possible differentiate septic from non-septic bursitis.
References:
Floemer F et al. MRI Characteristics of Olecranon Bursitis.AJR 2004: 183: 29-34
Student's elbow, Miner's elbow
Anatomy:
Several bursa occur in the posterior aspect of the elbow. Three common bursa occur and they include olecranon bursa (subcutaneous posterior to olecranon), deep intratendinoud bursa (within triceps near its insertion), deep subtendinous bursa (deep to triceps near insertion). Other uncommon bursae are subcutaneous medial and lateral epicondylar bursa, ulnar nerve bursa, subanconeous bursa.
Etiology:
Non-septic (2/3) : overuse, repeated traumatization (students, miners, American footballers), inflammatory arthropathy, obesity, uremia, RA, gout,
Septic (1/3): S.Auerus in 90%, rest in beta-hemolytic streptococcus. Riska include alcohol abuse, steroids, diabetes, renal impairment, malignancy
Clinical features:
Olecranon bursitis is a clinical diagnosis, and MRI is rarely performed. Clinical differentiation of septic and nonseptic bursitis may be difficult.
MRI:
Olecranon bursitis is a clinical diagnosis, and MRI is rarely performed. On Gd, rim enhancement is seen, even in non-septic bursitis. Associated features include joint effusion, soft tissue edema, thickened tricpes, bone marrow edema. It is not possible differentiate septic from non-septic bursitis.
References:
Floemer F et al. MRI Characteristics of Olecranon Bursitis.AJR 2004: 183: 29-34
shoulder: Parsonage-Turner Syndrome
Well-recognised uncommon condition with exact cause not known
Synonyms:
Brachial plexus neuritis, Patchwork amyotrophy, Localised neuritis of the shoulder girdle, Seratus magnus paralysis, Multiple neuritis of the shoulder girdle, Acute brachial radiculitis, Shoulder-girdle syndrome, Paralytic brachial neuritis, Acute shoulder neuritis, Acute scapula-humeral palsy, Brachial plexus neuropathy!!
Clinical features:
Sudden onset of pain across the top of the shoulder blade, lasts from a few hours to fortnight; followed by marked shoulder girdle muscle weakness and wasting and often arm. All patients may not recall pain. Wekness appears, pain stops. Sensation is preserved. May cause secondary shoulder impingement.
Investigations:
Nerve conduction studies - EMG.
Suprascapular nerve is almost invariably involved (97% ) , followed by axillary nerve (50%) and subscapular nerve is involved in only 3%.
Imaging:
Edema in the muscles of the shoulder girdle.
Fatty atrophy of the muscles
Treatment:
No specific treatment
Pain releif
Phisiotherapy and rehabilitation
Prognosis:
Generally good, about 75% recover completely in 2 years. Period of recovery varies from 6 months to 5 years.
References:
1. M. J. Parsonage, J. W. Aldren Turner:Neuralgic amyotrophy. The shoulder-girdle syndrome. The Lancet, London, 1948, I: 973-978.
2. Ryan M et al. Whole body magnetic resonance imaging in the diagnosis of Parsonage Turner syndrome. Acta Radiol. 2004 Aug;45(5):534-9. (PMID: 15515516)
3. Gaskin CM et al. Parsonage-Turner Syndrome: MR Imaging Findings and Clinical Information of 27 Patients. Radiology 2006 240: 501-507
Journal Watch:
1. Richard E et al. MRI Findings of 26 Patients with Parsonage-Turner Syndrome. AJR 2007;189:39-44
Synonyms:
Brachial plexus neuritis, Patchwork amyotrophy, Localised neuritis of the shoulder girdle, Seratus magnus paralysis, Multiple neuritis of the shoulder girdle, Acute brachial radiculitis, Shoulder-girdle syndrome, Paralytic brachial neuritis, Acute shoulder neuritis, Acute scapula-humeral palsy, Brachial plexus neuropathy!!
Clinical features:
Sudden onset of pain across the top of the shoulder blade, lasts from a few hours to fortnight; followed by marked shoulder girdle muscle weakness and wasting and often arm. All patients may not recall pain. Wekness appears, pain stops. Sensation is preserved. May cause secondary shoulder impingement.
Investigations:
Nerve conduction studies - EMG.
Suprascapular nerve is almost invariably involved (97% ) , followed by axillary nerve (50%) and subscapular nerve is involved in only 3%.
Imaging:
Edema in the muscles of the shoulder girdle.
Fatty atrophy of the muscles
Treatment:
No specific treatment
Pain releif
Phisiotherapy and rehabilitation
Prognosis:
Generally good, about 75% recover completely in 2 years. Period of recovery varies from 6 months to 5 years.
References:
1. M. J. Parsonage, J. W. Aldren Turner:Neuralgic amyotrophy. The shoulder-girdle syndrome. The Lancet, London, 1948, I: 973-978.
2. Ryan M et al. Whole body magnetic resonance imaging in the diagnosis of Parsonage Turner syndrome. Acta Radiol. 2004 Aug;45(5):534-9. (PMID: 15515516)
3. Gaskin CM et al. Parsonage-Turner Syndrome: MR Imaging Findings and Clinical Information of 27 Patients. Radiology 2006 240: 501-507
Journal Watch:
1. Richard E et al. MRI Findings of 26 Patients with Parsonage-Turner Syndrome. AJR 2007;189:39-44
case of the week: semimembranosus tear
History:
28 year old young gentleman was referred from the GP as requested by the orthopod for the ultrasound of the right knee. The patient had a football injury (possibly pivot-shift) more than a year ago which was evaluated with MRI of knee. The MRI of the knee reported tear in the anterior horn of the lateral meniscal.
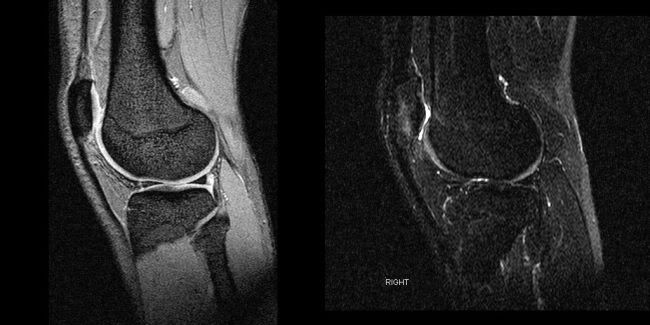
He underwent orthoscopy and meniscal repair. Despite the treatment, he continued to have pain on the posteromedial aspect of the knee which was worsening. Ultrasound was requested for further evaluation.
Image gallary:
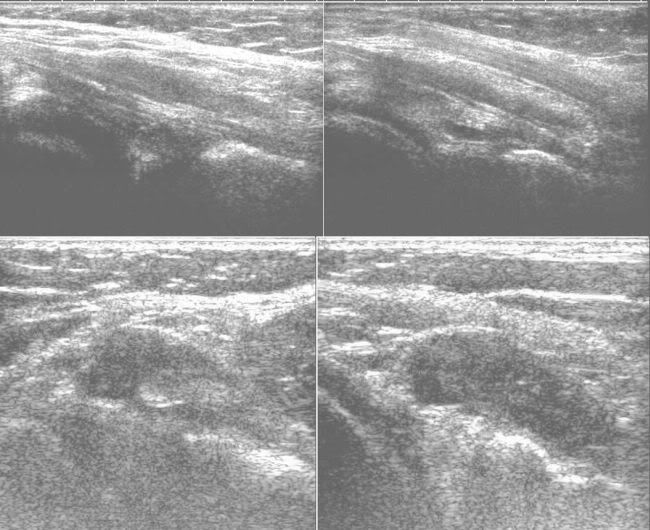
Imaging findings:
ULtrasound of the posteromedial aspect of the knee showed partial tear within the semimembranosus musculotendinous junction, extending up to the insertion with fluid around the tendon.
MR image review: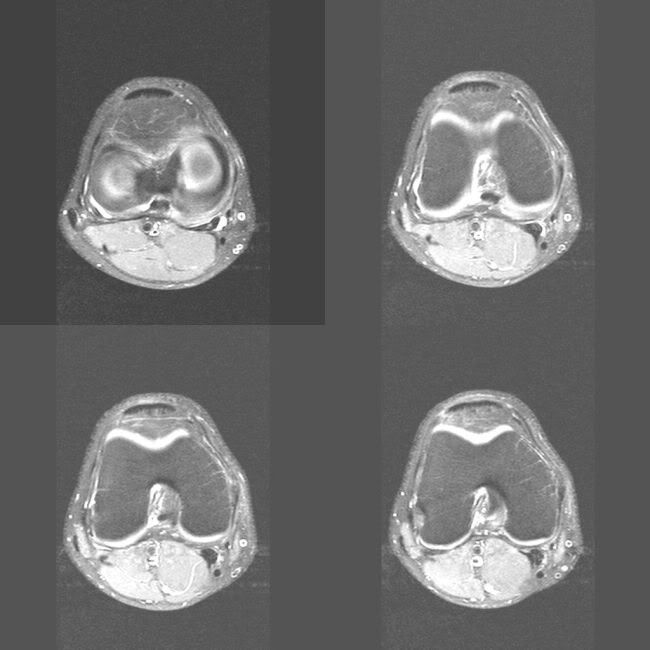
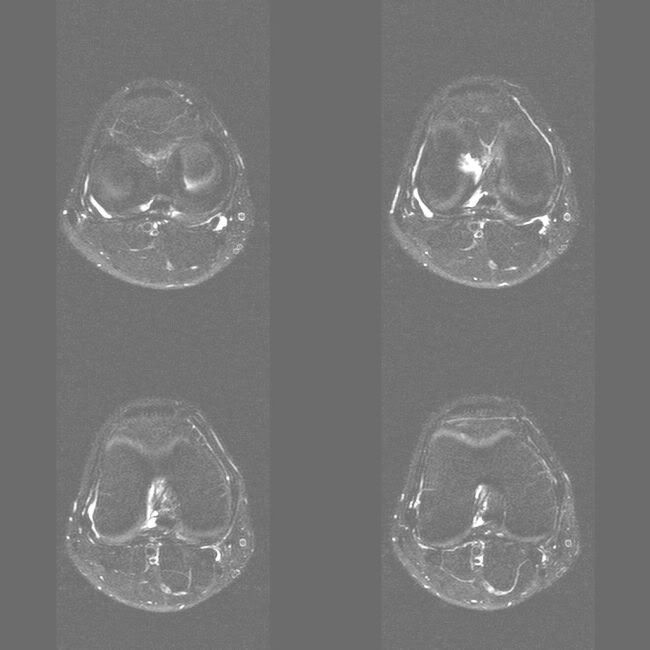
Review of the axial MR images also showed partial tear within the semimembranosus tendon with fluid around it. Actaully the appearances are virtually unchanged since the previous study.
Discussion:
Semimembranosus and semitendinosus are medial hamstrings (biceps is lateral hamstring). Their action is flexion and medial rotation of knee. Semimembranosus has a tendinous origin from the ischial tuberosity, crosses deep to semitendinosus and long head of biceps as a fusiform bulk, and inserts as a tendon in a complex fashion as 5 digital expansion: 1. main arm to posteromedial tibial plateau (infraglenoid tubercle) 2. oblique popliteal ligament 3. posteromedial capsule and posterior horn of medial meniscus 4. posterior oblique ligament 5. aponeurosis of popliteus muscle. Also it attaches to the superficial fibers of the medial collateral ligament. Recently the attachment to the posterior horn of the lateral meniscus is documented
The fusiform bulk is prone for strain injury. Partial tears of the medial head of the gastrocnemius at its origin is associated with semimembranosus strain injury. Avulsion injury of the main arm of insertion results from valgus stress and is associated with tears of the ACL and posterior horn of the medial meniscus.
This is a rare case of partial tear to the semimembranosus insertion associated with anterior horn of the lateral meniscus. Semimembranosus tendon is known to attach to posterior horn of the lateral meniscus. The association between posterior horn of the lateral meniscal tear and semimembranosus insertion tear has not been documented in the literature.
References:
1. Koulouris G et al. Evaluation of the hamstring muscle complex following acute injury.Skeletal Radiol 2003 Oct;32(10):582-9. (PMID: 12942206 )
2. Alioto RJ et al. Complete rupture of the distal semimembranosus complex in a professional athlete. Clin Orthop Relat Res 1997 Mar;(336):162-5 (PMID: 9060501)
3. Ray JM et al. Semimembranosus tendinitis: an overlooked cause of medial knee pain.Am J Sports Med 1988 Jul-Aug;16(4):347-51 (PMID: 3189658)
4. Bencard JT et al. Traumatic Musculotendinous Injuries of the Knee: Diagnosis with MR Imaging. RadioGraphics 2000; 20: 103
5. Kim YC et al. Tendinous insertion of semimembranosus muscle into the lateral meniscus.Surg Radiol Anat. 1997;19(6):365-9. (PMID: 9479710)
28 year old young gentleman was referred from the GP as requested by the orthopod for the ultrasound of the right knee. The patient had a football injury (possibly pivot-shift) more than a year ago which was evaluated with MRI of knee. The MRI of the knee reported tear in the anterior horn of the lateral meniscal.
He underwent orthoscopy and meniscal repair. Despite the treatment, he continued to have pain on the posteromedial aspect of the knee which was worsening. Ultrasound was requested for further evaluation.
Image gallary:
Imaging findings:
ULtrasound of the posteromedial aspect of the knee showed partial tear within the semimembranosus musculotendinous junction, extending up to the insertion with fluid around the tendon.
MR image review:
Review of the axial MR images also showed partial tear within the semimembranosus tendon with fluid around it. Actaully the appearances are virtually unchanged since the previous study.
Discussion:
Semimembranosus and semitendinosus are medial hamstrings (biceps is lateral hamstring). Their action is flexion and medial rotation of knee. Semimembranosus has a tendinous origin from the ischial tuberosity, crosses deep to semitendinosus and long head of biceps as a fusiform bulk, and inserts as a tendon in a complex fashion as 5 digital expansion: 1. main arm to posteromedial tibial plateau (infraglenoid tubercle) 2. oblique popliteal ligament 3. posteromedial capsule and posterior horn of medial meniscus 4. posterior oblique ligament 5. aponeurosis of popliteus muscle. Also it attaches to the superficial fibers of the medial collateral ligament. Recently the attachment to the posterior horn of the lateral meniscus is documented
The fusiform bulk is prone for strain injury. Partial tears of the medial head of the gastrocnemius at its origin is associated with semimembranosus strain injury. Avulsion injury of the main arm of insertion results from valgus stress and is associated with tears of the ACL and posterior horn of the medial meniscus.
This is a rare case of partial tear to the semimembranosus insertion associated with anterior horn of the lateral meniscus. Semimembranosus tendon is known to attach to posterior horn of the lateral meniscus. The association between posterior horn of the lateral meniscal tear and semimembranosus insertion tear has not been documented in the literature.
References:
1. Koulouris G et al. Evaluation of the hamstring muscle complex following acute injury.Skeletal Radiol 2003 Oct;32(10):582-9. (PMID: 12942206 )
2. Alioto RJ et al. Complete rupture of the distal semimembranosus complex in a professional athlete. Clin Orthop Relat Res 1997 Mar;(336):162-5 (PMID: 9060501)
3. Ray JM et al. Semimembranosus tendinitis: an overlooked cause of medial knee pain.Am J Sports Med 1988 Jul-Aug;16(4):347-51 (PMID: 3189658)
4. Bencard JT et al. Traumatic Musculotendinous Injuries of the Knee: Diagnosis with MR Imaging. RadioGraphics 2000; 20: 103
5. Kim YC et al. Tendinous insertion of semimembranosus muscle into the lateral meniscus.Surg Radiol Anat. 1997;19(6):365-9. (PMID: 9479710)
technique: ultrasound of the shoulder
Beware of anisotrophy all the time
Tendons are hyperechoic and ligaments are hypoechoic
Biceps:
Transverse:
Internal rotation, elbow 90 flexion
Scroll up and down, keeping the probe perpendicular to the tendon.
Look for: change in the calibre of the tendon (hyperechoic); fluid around the tendon (may be normal in the inferior aspect); subluxation on dynamic scan; transverse ligament (hypoechoic band)
Longitudinal:
Apply little pressure at the distal end to bring the tendon in longitudinal plane
Subscapularis and subscapularis bursa:
Inserts along the medial edge of the bicepital groove
Transverse:
External rotation, elbow 90 flexion, dynamic evaluation
Long axis:
Multipinnate appearance
Supraspinatus and subacromian-subdeltoid bursa:
Anatomical transverse/ long axis view:
Best to good postions (in order): Full adduction and internal rotation - place the hand against the back or 'place your hand as if you are putting it in your back pocket' or hanging arm with palm pointing backwards
Anterior postion: for anterior free edge ( at the corner corocoid process is seen), just lateral to biceps tendon. Most medial aspect is free edge. If there is gap between two, it indicates tear
Tears are best seen in this view
Mid position: lateral to the above view. Good for midsubstance tears.
Posterior position: Supraspinatus meets infraspinatus
Anatomical coronal/ oblique long axis:
Probe rests on the angle of the shoulder flat
Tendon seen as triangle
Infraspinatus:
Hand kept on the opposite shoulder
Posteromedial long axis positioning of the probe
Coracoacromial ligament:
Lateral to the free edge of the supraspinatus in transverse plane (long axis of supraspinatus). The ligament is seen as a low echoic band superior to the supraspinatus going towards corocaoid process
Acromioclavicular joint:
Feel and keep the probe
Glenohumoral joint:
Posteromedial to the infraspinatus view
References:
1. McNally EG. Practical musculoskeletal ultrasound. Churchill Livingstone 2005
Tendons are hyperechoic and ligaments are hypoechoic
Biceps:
Transverse:
Internal rotation, elbow 90 flexion
Scroll up and down, keeping the probe perpendicular to the tendon.
Look for: change in the calibre of the tendon (hyperechoic); fluid around the tendon (may be normal in the inferior aspect); subluxation on dynamic scan; transverse ligament (hypoechoic band)
Longitudinal:
Apply little pressure at the distal end to bring the tendon in longitudinal plane
Subscapularis and subscapularis bursa:
Inserts along the medial edge of the bicepital groove
Transverse:
External rotation, elbow 90 flexion, dynamic evaluation
Long axis:
Multipinnate appearance
Supraspinatus and subacromian-subdeltoid bursa:
Anatomical transverse/ long axis view:
Best to good postions (in order): Full adduction and internal rotation - place the hand against the back or 'place your hand as if you are putting it in your back pocket' or hanging arm with palm pointing backwards
Anterior postion: for anterior free edge ( at the corner corocoid process is seen), just lateral to biceps tendon. Most medial aspect is free edge. If there is gap between two, it indicates tear
Tears are best seen in this view
Mid position: lateral to the above view. Good for midsubstance tears.
Posterior position: Supraspinatus meets infraspinatus
Anatomical coronal/ oblique long axis:
Probe rests on the angle of the shoulder flat
Tendon seen as triangle
Infraspinatus:
Hand kept on the opposite shoulder
Posteromedial long axis positioning of the probe
Coracoacromial ligament:
Lateral to the free edge of the supraspinatus in transverse plane (long axis of supraspinatus). The ligament is seen as a low echoic band superior to the supraspinatus going towards corocaoid process
Acromioclavicular joint:
Feel and keep the probe
Glenohumoral joint:
Posteromedial to the infraspinatus view
References:
1. McNally EG. Practical musculoskeletal ultrasound. Churchill Livingstone 2005
case of the week
Shoulder:
Recurrent anterior shoulder dislocation
Elbow:
Calcific lateral epicondylitis and OA
Pelvis:
Pagets disease
Hip:
Hip pain
Knee:
Semimembranosus tear
Recurrent anterior shoulder dislocation
Elbow:
Calcific lateral epicondylitis and OA
Pelvis:
Pagets disease
Hip:
Hip pain
Knee:
Semimembranosus tear
case of the week: calcific lateral epicondylitis and OA elbow
History: 68 year old right handed lady presented with painful elbows with reduced range of movements. There was no history of other joint pain. The inflammatory markers were within normal limits. The rheumatoid factor was negative. The elbow radiographs showed osteoarthritic changes in both elbow joints, very severe in the right elbow. Few loose bodies were also seen. CT scan of the albow was done to further assess the loose bodies and osteoarthritis.
Image Gallary:


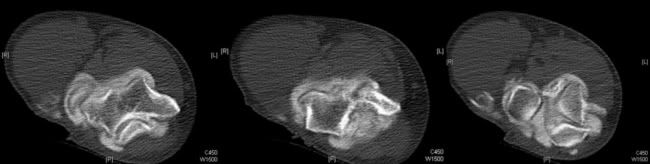
Imaging findings:
CT scan showed marked narrowing of the joint space with excessive bone formation in and around the elbow joint. Few loose bodies were also shown in the superior aspect of the joint. In addition, calcification was demostrated along the common extensor origin, which is suggestive of calcific lateral epicondylitis.
Discussion:
Osteoarthtitis of the elbow:
Osteoarthritis of the elbow joint is not common. Primary osteoarthitis is almost exclusively seen in men. Although trauma is one of the causes for the osteoarthritis of the elbow joint, many times history of trauma is not elicited. Injury to the ligaments resulting in an unstable elbow can also lead to arthritis, even if the elbow surface is not damaged. For example, professional baseball pitchers place unusually high demands on their throwing elbows.
Plain radiographs usually show spurs at the anterior end of the coronoid and posterior margin of olecranon. CT or MRI are used to differentiate loose bodies from osteophytes. Loss of articular cartilage is common in radiohumeral joint than ulnohumeral joint. Chondral defects tend to occur in the posterolateral aspect of the trochlear notch in sports related osteoarthritis.
Intially the degenerative joint is managed conservatively. Surgical options include arthoscopic debridement, interpostion arthroplasty (tendon or fascia between articular surfaces), radial head excision, orthodesis and elbow joint replacement.
Calcific lateral epicondylitis:
Lateral epicondylitis is a very common overuse syndrome and has many acronyms, viz., tennis elbow, plasterer's elblow, mechanic's elblow, painter's elbow. It is due to overusage of the common extensors of the elbow. According to Nirschl and Pettrone it is due to microscopic tears and reparative tissue in the origin of the extensor carpi radialis brevis (ECRB) muscle. Nirschl also staged the injury: Stage 1 - reversible inflammatory changes. Stage 2 - non-reversible in the origin of the ECRB, Stage 3 - rupture of ECRB, Stage 4 - secondary changes like fibrosis or calcification (calcific lateral epicondylitis)
Plain radiographs may show osteophytes over the lateral epicondyle, calcification close to the lateral epicondyle.
US of the common extensor tendon had high sensitivity but low specificity in the detection of symptomatic lateral epicondylitis
MR is used frequently in the evaluation. Tendinosis is seen as a thickening of the tendon with intermediate signal on T1WI. Mucoid degenerations show high signal T2WI. Coronal or oblique coronal cuts are helpful in the assessment.
CT is not used in the evaluation of the lateral epicondylitis and in the present case it was incidentally diagnosed.
References:
Teh J et al. Imaging of the elbow. Imaging 15:193-204 (2003)
Levin D et al. Lateral Epicondylitis of the Elbow: US Findings. Radiology 2005;237:230-234
Image Gallary:
Imaging findings:
CT scan showed marked narrowing of the joint space with excessive bone formation in and around the elbow joint. Few loose bodies were also shown in the superior aspect of the joint. In addition, calcification was demostrated along the common extensor origin, which is suggestive of calcific lateral epicondylitis.
Discussion:
Osteoarthtitis of the elbow:
Osteoarthritis of the elbow joint is not common. Primary osteoarthitis is almost exclusively seen in men. Although trauma is one of the causes for the osteoarthritis of the elbow joint, many times history of trauma is not elicited. Injury to the ligaments resulting in an unstable elbow can also lead to arthritis, even if the elbow surface is not damaged. For example, professional baseball pitchers place unusually high demands on their throwing elbows.
Plain radiographs usually show spurs at the anterior end of the coronoid and posterior margin of olecranon. CT or MRI are used to differentiate loose bodies from osteophytes. Loss of articular cartilage is common in radiohumeral joint than ulnohumeral joint. Chondral defects tend to occur in the posterolateral aspect of the trochlear notch in sports related osteoarthritis.
Intially the degenerative joint is managed conservatively. Surgical options include arthoscopic debridement, interpostion arthroplasty (tendon or fascia between articular surfaces), radial head excision, orthodesis and elbow joint replacement.
Calcific lateral epicondylitis:
Lateral epicondylitis is a very common overuse syndrome and has many acronyms, viz., tennis elbow, plasterer's elblow, mechanic's elblow, painter's elbow. It is due to overusage of the common extensors of the elbow. According to Nirschl and Pettrone it is due to microscopic tears and reparative tissue in the origin of the extensor carpi radialis brevis (ECRB) muscle. Nirschl also staged the injury: Stage 1 - reversible inflammatory changes. Stage 2 - non-reversible in the origin of the ECRB, Stage 3 - rupture of ECRB, Stage 4 - secondary changes like fibrosis or calcification (calcific lateral epicondylitis)
Plain radiographs may show osteophytes over the lateral epicondyle, calcification close to the lateral epicondyle.
US of the common extensor tendon had high sensitivity but low specificity in the detection of symptomatic lateral epicondylitis
MR is used frequently in the evaluation. Tendinosis is seen as a thickening of the tendon with intermediate signal on T1WI. Mucoid degenerations show high signal T2WI. Coronal or oblique coronal cuts are helpful in the assessment.
CT is not used in the evaluation of the lateral epicondylitis and in the present case it was incidentally diagnosed.
References:
Teh J et al. Imaging of the elbow. Imaging 15:193-204 (2003)
Levin D et al. Lateral Epicondylitis of the Elbow: US Findings. Radiology 2005;237:230-234
Subscribe to:
Posts (Atom)